
Note to myself and my readers: As always the Curbsiders’ show notes for this episode [and all episodes] are outstanding. I just post these excerpts to help fix the episode in my mind.
It is best for me, and I think other learners, to review the actual show notes which have much more detail.
Links to and excerpts from The Curbsiders‘ [Link is to the complete episode list] January 25, 2021, #252 Smoking Cessation Unfiltered, By :
Breaking the Chain with Medications and Behavioral Interventions
Summary
Get all the details on varenicline, nicotine replacement therapy, and integrating psychosocial interventions into a comprehensive smoking cessation treatment plan! Smoking cigarettes is the leading cause of preventable death worldwide. Listen as our esteemed guest Dr. Steve Baldassarri (Yale University School of Medicine) provides us expert pearls to help our patients quit smoking.
Here is the podcast:
Here are excerpts:
Smoking Cessation Unfiltered Pearls
- Daily cigarette smoking is an addiction and is considered a chronic disease. It typically follows a relapsing-remitting course for individuals similar to other chronic diseases.
- Obtain a tobacco use history by asking individuals about their age of first use, duration, number of cigarettes a day, prior treatments, and time to first cigarette in the morning.
- Time to first cigarette use in the morning is a good predictor of nicotine dependence (Baker, 2007). Selecting a starting dose of nicotine gum, is based on time to first cigarette (TTFC) upon waking. If the TTFC is > 30 minutes, select the 2 mg nicotine gum, if TTFC is < 30 minutes, select the 4mg gum.
- Assess a patient’s motivation for smoking cessation by using motivational interviewing techniques and by asking an open-ended question such as “how do you feel about your tobacco use?”.
- A comprehensive smoking cessation care plan should be patient centered, and include pharmacotherapy, behavioral interventions and close follow-up with health care providers.
- If monotherapy is chosen, varenicline is superior to bupropion for smoking cessation (Nides, 2008). Consider the use of bupropion for patients with co-morbid depression, or those concerned about smoking cessation weight gain.
- The presence of a well-controlled psychiatry diagnosis is not a contraindication to take varenicline, bupropion, or nicotine replacement therapy (NRT) (Anthenelli, 2016).
- Do not withdraw pharmacotherapy (eg: NRT or varenicline) if a patient is not abstinent. Instead consider adding additional treatment such as psychosocial interventions, and adding or dose adjusting additional pharmacotherapy.
- The diagnosis of E-cigarette or Vaping Use Associated Lung Injury (EVALI), notably has been described in both THC and nicotine based products (CDC EVALI Reports – Chinai, 2020).
- If standard treatments do not work for smoking cessation, patients may choose to use electronic cigarettes or vapes as a harm reduction strategy. Vaping is likely much less harmful than smoking, but may still cause health problems. Counsel the patient to avoid the use of any combustible products if they choose to vape.
Smoking Cessation Unfiltered Notes
Tobacco Use Disorder Overview
Many individuals who smoke cigarettes develop a tobacco use disorder. Nicotine is the cigarette’s primary addictive chemical, but there are many other factors that influence addiction to cigarettes.
Smoking is the leading cause of preventable death worldwide (CDC Tobacco Use). We view cigarette addiction as a chronic disease that has a relapsing and remitting course for patients.
- Ask about tobacco use at every visit.
- Advise to quit in a clear and personalized manner.
- Assess willingness to quit.
- Assist in quitting.
- Arrange follow-up and support.
FACTORS ASSOCIATED WITH CHALLENGES IN SMOKING CESSATION
There are a variety of factors associated with successful and failed smoking quit attempts. Factors such as early age of onset, time to first cigarette in the morning, presence of an existing mood disorder, and coexisting substance use (e.g. alcohol) may lead to higher rates of failed smoking quit attempts or higher rates of return to use (Greenhalgh, 2016). In addition, there are high rates of tobacco use among individuals with comorbid psychiatric and substance use disorders compared to individuals without these diagnoses ( Kalman, 2005).
ABRUPT CESSATION VS. GRADUAL REDUCTION
Patients may opt to quit abruptly, or they may opt for a gradual reduction in their cigarette use. Dr. Baldassarri’s expert advice is that there is “ one size fits” all for patients, and clinicians should ask a patient which strategy they think will work best for them. In his expert opinion if a patient has factors associated with more significant nicotine dependence, then they may be more successful with a gradual reduction in their cigarette use. Setting quit dates can be used as an approach for patients who opt for abrupt cessation.
NICOTINE WITHDRAWAL
Stopping nicotine abruptly can cause an individual to develop symptoms of nicotine withdrawal. Symptoms such as mood disturbances, increased appetite, irritability, fatigue, and trouble sleeping may occur (DSM-V Tobacco Withdrawal). A patient may experience a range in severity of these symptoms, and utilizing pharmacotherapy can minimize a patient’s symptoms of nicotine withdrawal.
Prescribing Pharmacotherapy
Patients should be prescribed at least 1 long acting, “controller” medication as a first line therapy and notably they can be used in combination (e.g.: varenicline and nicotine patch). Add short acting nicotine replacement to help control cravings.
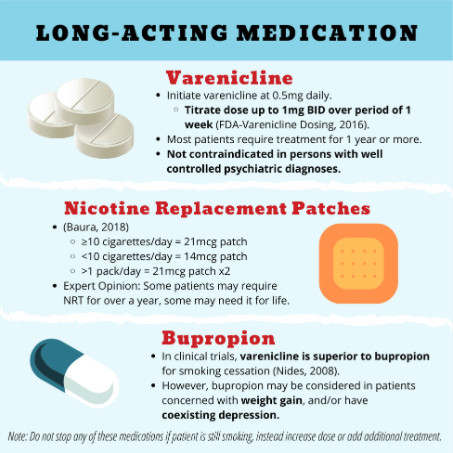
There are 3-FDA approved long-acting medications: the nicotine replacement patch (full agonist of nicotinic receptor), varenicline (partial agonist of nicotinic receptor), and bupropion (antidepressant in the aminoketone class).
Varenicline
Initiate varenicline at 0.5mg daily, then titrate the dose up to 1mg BID over a period of 1 week to ensure the medication side effects are minimal (FDA-Varenicline Dosing). Common side effects include nausea, vivid dreams, insomnia but generally are mild and well tolerated. Duration of use should occur for a minimum of 3 months, but most patients will benefit from long term use of this medication. Dr. Baldassarri’s expert opinion is that most patients will require 1 year or more of this therapy. Even if an individual is not abstinent from cigarettes, they can continue this medication. Do not stop varenicline if a patient is still smoking, instead add additional treatment options such as nicotine replacement therapy (NRT) or behavioral interventions.
The presence of a well-controlled psychiatric diagnosis is not a contraindication to take varenicline (or bupropion, or NRT). The EAGLES trial did not show a significant increase in neuropsychiatric adverse events attributable to varenicline or bupropion relative to nicotine patch or placebo (Anthenelli, 2016). Dr. Baldassarri still recommends monitoring for symptoms such as depression, and suicidal thoughts during treatment, and after cessation of these medications.
Nicotine Replacement Therapy – Patches
NRT can minimize the symptoms of nicotine withdrawal. To determine the optimal dosing of a nicotine patch, a provider must estimate an individual’s daily nicotine consumption based on the number of cigarettes they smoke a day (Baura, 2018).
Dosing: Guidelines suggest prescribing a 21mcg patch if an individual smokes 10 or more cigarettes a day, and using a 14mcg patch if they smoke less than 10 cigarettes a day (Baura, 2018). Number of cigarettes smoked a day is only a rough estimate of total nicotine consumption because there is variability in how individuals smoke. In Dr. B’s expert opinion, NRT is often underdosed. For an individual who smokes more than 1 pack per day, starting with two-21mcg patches (42 mg) is likely to better control their symptoms of withdrawal. Remember to be flexible in dosing, and it is ok to increase a NRT patch dose if a patient describes symptoms of nicotine withdrawal.
Counseling: Individuals should change a NRT patch every 24 hours. Emphasize to the patient that it takes 2-4 days for a nicotine patch to reach steady state (Gorsaline, 1993). If a patient is still smoking with the patch on, they should keep it on and NOT remove it. Smoking while on a NRT patch signals inadequate control of nicotine withdrawal or cravings. Consider increasing the NRT patch dosage, or prescribing additional short acting NRT gum or lozenges up to every 15 or 30 minutes.
Duration of NRT patches: Guidelines state that the typical duration is 3 weeks, and expert opinion is to continue them for longer periods of time, until an individual is confident, they will not return to cigarette use (Baura, 2018). NRT patches are safe to use for at least 1 year with no harms reported (Schnoll, 2015). Dr. Baldassarri recommends that if a NRT patch is working, do not change it quickly, and to taper the medication very slowly, if at all. He states that some patients may require NRT replacement for over a year, and some may need it for life. Safety data beyond a year of use is limited, and a clinician should balance the risks of the medication vs. long term use.
Smoking while on NRT: The risk of nicotine toxicity is possible, but it is very rare. Common symptoms of nicotine toxicity include nausea, vomiting, palpitations, lightheaded, and dizziness. Remind individuals experiencing mild symptoms to not take off the patch, but instead stop cigarettes.
Bupropion
Studies have demonstrated that varenicline is superior to bupropion for smoking cessation, yet there may be specific patients that prefer this pharmacotherapy (Nides, 2008). Side effects of bupropion include weight loss, lower seizure threshold, insomnia and dry mouth. For patients who are concerned about the weight gain after smoking cessation, and/or have coexisting depression, consider the utilization of this medication.

Utilizing short acting NRT as “PRNs” may help control cigarette cravings, examples include nicotine based: gum, lozenge, inhaler, or intranasal spray. It is important to counsel patients that tobacco cravings can last from months to years. The intranasal spray delivers nicotine the fastest (peak plasma levels in 15 minutes), but often is poorly tolerated due to side effects such as nasal burning, throat burning (Houezec, 2003). The gum reaches peak nicotine levels within 1 hour, yet a cigarette can reach peak nicotine levels within 5 minutes (Houezec, 2003). These agents should be used in conjunction with long-acting medications such as NRT patches, varenicline, or bupropion. Bupropion can be combined safely with any of the other smoking cessation medications including varenicline and NRT.
Nicotine Gum Dosing: The guidelines recommend selecting a dose of nicotine gum based upon the time to first cigarettes in the morning (Baura, 2018). If time to first cigarette upon waking is less than 30 minutes, prescribe the 4mg nicotine gum, if it is greater than 30 minutes after waking up, utilize the 2mg gum (Baura, 2018). Expert tip, per Dr. Baldassarri most patients will require the 4mg dosing.
Behavioral Interventions
Behavioral interventions can increase the odds of a successful quit attempt (Siu, 2015). Resources will vary locally, and remember that stress can be a major contributor to continued tobacco use and relapse (Cohen, 1990). Referring a patient to a social worker may be an important part of a patient’s smoking cessation care plan to address life stressors. Be aware of your local resources. Behavioral interventions in a dose dependent fashion have been found to increase successful quit attempts (Siu, 2015). Telephone quitlines, cognitive behavioral therapy, and group classes, are some examples of interventions that can be added to a patient’s care plan. More intensive and supportive behavioral interventions tend to produce better results.
See the show notes for the author’s thoughts on Vaping and Electronic Cigarettes.
EVALI
The diagnosis of E-cigarette or Vaping Use Associated Lung Injury (EVALI), notably has been described in both cannabis and nicotine products. The majority of cases were associated with cannabis and vitamin E acetate (CDC EVALI Reports – Chinai, 2020). Further research is needed to better understand product risk factors for EVALI.
Take Home Point
Smoking cessation is challenging, and we need to be positive, non-judgmental, patient, empathetic, persistent and support our patients in their smoking cessation journey.



