
In addition to Dr. Farkas’ chapter below, please see
- EMRA PRESSORDEX, 4TH EDITION, 2020 [Not an affiliate link. I just strongly recommend the book.]
- “When you’re managing critically ill patients, time matters. Make the most of it with EMRA PressorDex®: Critical Care Medication Guide, the best on-shift guide to pressors, vasoactive drugs, continuous infusions, and other medications. This indispensable pocket resource helps you choose the right medication and dosages, even during the busiest ICU shift. Researched by 100 critical care specialists and pharmacy faculty from 35 institutions around the country, this guide offers evidence-based options you can trust.”
- Wellington ICU Drug Manual, 2020. v3a.
- About this website
- “All Content © 2011-20 WellingtonICU.com”
- “This formulary is the online version of the Wellington ICU Drug Manual developed by Drs.Paul Young & Alex Psirides for use in the Intensive Care Unit of Wellington Regional Hospital. It has been specifically developed for use on portable devices (smartphones & tablets) at the bedside.”It is based on the Third Edition of the printed manual which is also available as a PDF for offline usage. The manual was originally developed in 2011 as a reference aid for the medical & nursing staff of Wellington ICU and reflects common ICU practice, both local and elsewhere.”
In this post I link to and excerpt from The Internet Book Of Critical Care [link is to the Table Of Contents] chapter, Generalized Convulsive Status Epilepticus, February 8, 2020 by Josh Farkas.
All that follows is from the above IBCC chapter.
CONTENTS
- Diagnosis & definition
- Causes
- Investigation
- Treatment
- Algorithm
- Podcast
- Questions & discussion
- Pitfalls
- PDF of this chapter (or create customized PDF)
definition of status epilepticus
generalized status epilepticus requires both:
- (1) Generalized seizure: The seizure should cause diffuse motor activity and loss of consciousness. This distinguishes it from a partial seizure (e.g. movement of one extremity with retention of consciousness). This is important because partial status epilepticus (“epilepsia partialis continua”) can be treated less aggressively.
- (2) Either one of the following:
- i) A single seizure which lasts for >5 minutes (self-terminating seizures generally last <5 minutes).
- ii) Multiple seizures without regaining normal mental status in-between.
differentiation from pseudoseizure
evaluation and management
- When in doubt, video EEG capture can help make these distinctions.
- If a diagnosis can’t be made with certainty, the safest approach can be to treat these as genuine seizures (e.g. with benzodiazepine).
causes
metabolic
- Hyponatremia/hypernatremia
- Hypoglycemia/hyperglycemia (hyperglycemia may tend to cause focal seizures)
- Hypophosphatemia
- Hypoxemia, respiratory alkalosis
- Uremia, dialysis disequilibrium
- Hyperammonemia (of any cause), hepatic encephalopathy
- Hyperthermia
malignancy
- Primary brain tumor (e.g. glioblastoma multiforme)
- Metastatic disease
infectious / inflammatory
- Meningitis, encephalitis (viral, paraneoplastic, anti-NMDA receptor encephalitis)
- Brain abscess
- Lupus, vasculitis
- Sepsis with systemic inflammation (may reduce seizure threshold)
vascular
- Remote stroke which caused residual epileptogenic focus.
- Acute stroke (ischemic > hemorrhagic).
- Hypertension-related:
- Hypertensive encephalopathy /Posterior Reversible Encephalopathy Syndrome (PRES)
- Eclampsia
traumatic brain injury
drugs
- (1) Non-adherence with anti-epileptic therapy, changes in regimen, drug-drug interactions
- (2) Medications that lower seizure threshold; more common examples:
- Psychiatric medications (antipsychotics; antidepressants, especially bupropion or tricyclics; lithium)
- Local anesthetics (e.g. lidocaine)
- Antimicrobials (e.g. beta-lactams, quinolones, metronidazole, acyclovir, gancyclovir, isoniazid)
- Antihistamines, baclofen
- Ancient analgesics (tramadol, meperidine, propoxyphene)
- Chemotherapeutics & immunomodulators (e.g. cisplatin, methotrexate, tacrolimus, cyclosporine)
- Theophylline
- Withdrawal of benzodiazepines, barbiturates, baclofen, or gabapentin.
- (3) Toxicologic
- Withdrawal from alcohol or benzodiazepine
- Overdose with sympathomimetic, salicylate, tricyclic, anticholinergic, lithium, synthetic cannabinoids
status epilepticus without an obvious cause? think NORSE
NORSE (new-onset refractory status epilepticus)
- Definition: Refractory status epilepticus without any readily identifiable cause (in a patient without prior seizures or structural neurologic disease).
- Causes:
- ~40% Non-paraneoplastic autoimmune (e.g. anti-NMDA encephalitis)
- ~30% Paraneoplastic
- ~20% Infectious
investigation
history
- Careful review of medication list, including any recent changes (look up drugs individually to determine if they lower seizure threshold).
- ? Preceding febrile illness or other complaints.
- ? Use of alcohol or other substances.
- ? Seizure initiated with focal symptoms, with subsequent generalization (this suggests focal neurologic pathology).
neuro exam
- Immediately following the seizure, patients may have focal neurologic defects in areas involved in the seizure (Todd’s Paralysis).
- Prompt examination is important, as findings may disappear over time.
- A focal abnormality on neurologic examination (e.g. asymmetric findings) suggests a focal neurologic lesion as the trigger of the seizure. This increases the importance of neuroimaging.
labs
- Basics
- Fingerstick glucose (should be done immediately).
- CBC, chemistries including Ca/Mg/Phos.
- Liver function tests, including ammonia level.
- Creatinine kinase (to evaluate for rhabdomyolysis due to seizures).
- Urinalysis, urine pregnancy test if relevant.
- Additional considerations
- Anti-epileptic drug levels (usually not available rapidly, but may be helpful later on to differentiate between nonadherence and medication failure).
- Toxicology workup as indicated (e.g. urine toxicology screen including cocaine and methamphetamine).
neuroimaging
- CT head generally indicated unless cause is obvious (e.g. non-adherence with anti-epileptic agents).
- MRI useful if etiology remains unclear.
lumbar puncture
- The main indication is usually exclusion of meningitis/encephalitis, if this is suspected clinically.
- Note that prolonged status epilepticus itself can cause elevation of protein and total cell count (but not above ~80-100 /mm3).
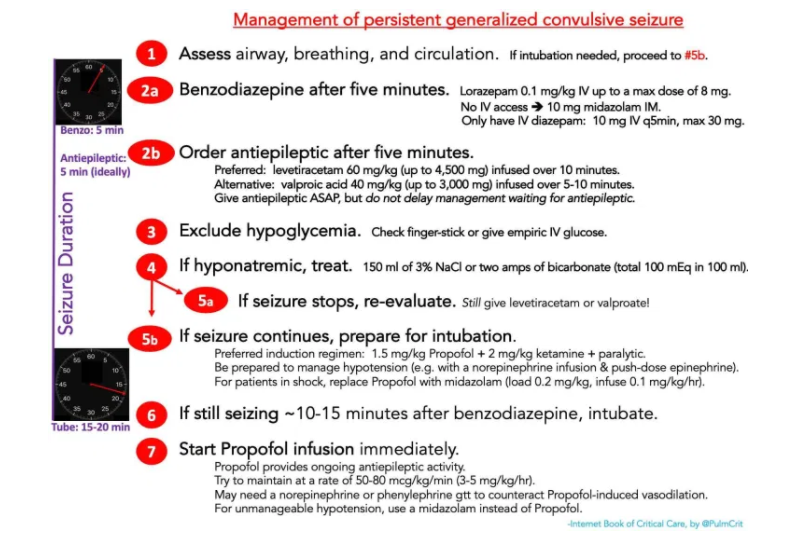
treatment algorithm
This algorithm describes the approach to a convulsive generalized seizure lasting >5 minutes. For a patient with recurrent seizures who isn’t actively seizing, a more gradual approach may be taken (with escalation if an active seizure resumes).
The duration of time in which a patient can be in convulsive status epilepticus before brain damage occurs is unknown. Many experts estimate this to be around 30 minutes (30516601). Consequently, the above algorithm is designed to break nearly all seizures within 30 minutes. This requires rapid escalation to intubation.
benzodiazepine is front-line therapy
dosing
- IV lorazepam is generally the preferred agent.
- The best research supports a dose of 0.1 mg/kg lorazepam IV (Treiman 1998).
- However, many guidelines recommend giving 4 mg IV initially, with a repeat dose if this isn’t effective. That may also be reasonable.
- For patients without IV access, give 10 mg intramuscular midazolam (Silbergieit 2011).
- Diazepam: 10 mg IV, may repeat q5-10 minutes to a maximum cumulative dose of 30 mg.
do not under-dose your benzodiazepine
- Over time, GABA receptors on neurons are internalized within cells. This reduces the sensitivity of the seizure to benzodiazepines.
- Up-front adequate dosing of benzodiazepine provides the best chance for immediate lysis of the seizure.
- Evidence does NOT support the concept that benzodiazepines for status epilepticus promote respiratory depression and intubation. In fact, adequate doses of benzodiazepines may reduce the need for intubation. One caveat here is that the clinician must be patient in allowing the postictal, post-benzodiazepine patient to wake up (these patients will have altered mental status, but by itself that’s not an indication for intubation).
don’t stop here!
- Even if the benzodiazepine breaks the seizure, you still need to give the patient a conventional anti-epileptic agent! More on this below.
hypoglycemia & hyponatremia
exclude hypoglycemia
- Hypoglycemia must be excluded in any patient with seizures or mental status changes.
- Usually a finger stick-glucose is adequate for this. However, if there is difficulty obtaining a finger-stick glucose or if the measurement is borderline, just give IV glucose empirically (1-2 ampules of D50W).
treat hyponatremia if present
- Hyponatremia is an uncommon cause of seizures. However, this is important because seizures due to hyponatremia should be treated with hypertonic saline immediately.
- Standard therapy would be a bolus of 150 ml 3% saline, which may be repeated once for ongoing seizure.
- Hypertonic saline often takes 15-20 minutes to arrive from pharmacy. In an emergency, 2 amps of bicarbonate (each amp equals 50 mEq bicarbonate in 50 ml) can be substituted for 150 ml of 3% saline (described further here).
conventional anti-epileptic
conventional anti-epileptic agent is indicated for ALL status epilepticus patients
- Any patient who seizes for >5 minutes should receive an anti-epileptic agent, even if benzodiazepine is successful in stopping the seizure. The benzodiazepine will last only for a few hours, so treatment with benzodiazepine alone leaves the patient at risk for delayed seizure recurrence.
- There is no reason to intentionally delay the conventional anti-epileptic agent until after the benzodiazepine (because it will be required regardless).
- For a patient with active convulsive seizures, don’t delay intubation while waiting for the anti-epileptic agent to arrive from the pharmacy.
- The anti-epileptic should be ordered ASAP and given as early as possible.
- If the anti-epileptic arrives from pharmacy
- and breaks the seizure within 20 minutes then intubation isn’t necessary. That would be terrific, but in most scenarios this is logistically impossible.
- Intubation shouldn’t be delayed while waiting to see if the second-line antiepileptic agent will work (target intubation by ~20 minutes after seizure initiation, regardless of whether or not the conventional anti-epileptic agent has arrived).
levetiracetam is the generally the preferred agent
- Benefits of levetiracetam:
- It has essentially no contraindications – so you can safely prescribe this to patients without knowing much about them.
- It can be infused rapidly.
- It is extremely safe; in particular, it is unlikely to cause alteration in consciousness (31766004).
- It has minimal interactions with other drugs.
- Contraindications: None
- Side-effects: Can cause mood disturbance, SIADH
- Dosing
- Loading dose: 60 mg/kg up to a max total dose of 4.5 grams, infused over 10 minutes.
- Maintenance dose: usually 1-1.5 grams IV q12hr (up to 2 grams IV q12 hr in selected cases).
valproic acid
- A reasonable option
- Contraindications
- Hyperammonemia, liver disease
- Pregnancy
- Thrombocytopenia, active bleeding
- Side-effects
- Thrombocytopenia, impaired platelet aggregation
- Pancreatitis, hepatotoxicity
- Hyperammonemic encephalopathy
- Stevens-Johnson Syndrome
- Drug reaction with eosinophilia and systemic symptoms (DRESS)
- SIADH
- Dosing
- Loading dose: 40 mg/kg (up to 3,000 mg) infused over 5-10 minutes. May give additional 20 mg/kg over 5 minutes.
- Maintenance dose: 30-60 mg/kg daily in divided doses, q12hr or q8hr.
- Monitoring
- Target serum level 80-140 mg/dL.
- Target free level of 4-11 ug/ml (obtain free level only if toxicity is suspected).
valproic acid
- A reasonable option
- Contraindications
- Hyperammonemia, liver disease
- Pregnancy
- Thrombocytopenia, active bleeding
- Side-effects
- Thrombocytopenia, impaired platelet aggregation
- Pancreatitis, hepatotoxicity
- Hyperammonemic encephalopathy
- Stevens-Johnson Syndrome
- Drug reaction with eosinophilia and systemic symptoms (DRESS)
- SIADH
- Dosing
- Loading dose: 40 mg/kg (up to 3,000 mg) infused over 5-10 minutes. May give additional 20 mg/kg over 5 minutes.
- Maintenance dose: 30-60 mg/kg daily in divided doses, q12hr or q8hr.
- Monitoring
- Target serum level 80-140 mg/dL.
- Target free level of 4-11 ug/ml (obtain free level only if toxicity is suspected).
fosphenytoin
- Reasons fosphenytoin isn’t generally preferred:
- It has numerous contraindications (e.g. pregnancy, hepatic dysfunction, renal dysfunction).
- It can cause bradycardia or hypotension (if given too rapidly, or to patients with cardiac comorbidity). Other potential complications include Stevens-Johnson Syndrome, pancytopenia, tissue necrosis if extravasation occurs, phlebitis, and drug fever.
- It causes numerous drug-drug interactions. In particular, it shouldn’t be used together with valproate (valproate inhibits CYP2C9, which leads to accumulation of phenytoin; valproate also competes for binding to albumin and thereby increases the free level of phenytoin).
- Monitoring phenytoin levels in the ICU is often impossible (unless your lab provides rapid turn-around time on free phenytoin levels).
- Toxic levels may cause delirium.
- Dosing
- Loading dose is 20 PE/kg at 100-150 PE/min (may give additional 5-10 PE/kg for ongoing seizures). Fosphenytoin is dosed in terms of “phosphenytoin equivalents” rather than mg.
- Maintenance dose is 5-7 PE/kg/day in 2-3 divided doses.
- Monitoring
- Target total level of ~15-25 ug/mL (but this isn’t very accurate for critically ill patients). This may be corrected for albumin if free fosphenytoin levels aren’t rapidly available (online calculator here).
- Ideally, a free phenytoin level may be checked, targeting a level of 2-3 ug/mL (especially in patients with renal dysfunction or other medications which compete with phenytoin for albumin binding).
- Check levels at least >2 hours after the last dose.
phenobarbital
- Not widely used, but may be helpful in specific situations:
- (1) Arguably the preferred anti-epileptic for alcohol withdrawal seizures. More on this here.
- (2) May be useful in super-refractory status epilepticus, to assist in weaning patients off a barbiturate coma.
loading dose for patients on chronic anti-epileptic therapy
- All patients with status epilepticus should be loaded with an anti-epileptic agent (usually levetiracetam, fosphenytoin, or valproate).
- For patients on one of these drugs previously:
- If the patient is believed to be adherent with therapy, it could make sense to load with a different drug. For example, a valproate load could be used in a patient on chronic levetiracetam.
- If the patient is felt to be potentially non-adherent, then re-loading with the patient’s chronic anti-epileptic could make sense.
- When in doubt, levetiracetam may be a good choice here, because supra-therapeutic levels are reasonably safe.
neurolytic intubation
preparation for intubation
- Propofol is generally the best induction drug here, given its potent anti-epileptic activity. The only exception would be a patient with severe hypotension (in whom midazolam provides more hemodynamic stability). Ketamine has anti-epileptic activity as well, which may function synergistically with propofol or midazolam (ketamine blocks NMDA receptors, while propofol blocks GABA receptors).
- The combination of sedation, vasodilation from propofol, and positive pressure ventilation may decrease the blood pressure. Be prepared for this (e.g. have a norepinephrine infusion and/or push-dose epinephrine ready).
- Regarding paralytic:
- Succinylcholine may be contraindicated in prolonged status epilepticus, as this may lead to rhabdomyolysis and hyperkalemia.
- Rocuronium causes prolonged paralysis, which may be problematic because it can mask ongoing seizure activity. However, sugammadex can be used following intubation to reverse paralysis and determine if there is residual seizure activity (if EEG isn’t readily available).
- Note that muscular paralysis won’t prevent brain damage from ongoing seizure activity. The goal is always to control the seizure itself, not to mask it using paralytics.
- Placement of a tourniquet on an extremity before paralysis may prevent paralytic from entering that extremity, thereby allowing you to determine if the seizure has been terminated.
example of a neurolytic intubation
- There are many ways to accomplish this. One strategy involves the following sequence of drugs:
- #1: Push 200 mg IV ketamine.
- #2: Push 100 mg of propofol (10 ml).
- #3: Push 0.6 mg/kg rocuronium (this is a lower dose than is usually used, so that it will take a bit longer to work than usual and won’t last too long).
- This will result in one of two outcomes:
- (#1) The ketamine and propofol will usually break the seizure. This results in an abrupt cessation of motor activity about 30-60 seconds after pushing the propofol (before the onset of paralysis). You can usually intubate the patient when that occurs – the patient is generally quite flaccid.
- (#2) The ketamine and propofol fail to break the seizure. In this case, seizure movements will gradually become less pronounced as paralysis occurs. Disappearance of all movement generally occurs >60 seconds after administration of rocuronium.
- Based on the dose and sequence of drugs used, the rocuronium isn’t generally really needed here (the propfol and ketamine will generally break the seizure and produce adequate intubating conditions). The rocuronium is merely an insurance policy so that in case the propofol and ketamine don’t break the seizure, you will still get adequate intubating conditions.
initiate sedative infusion (propofol)
- Propofol (+/- ketamine) will generally break the seizure. However, an ongoing infusion of propofol is still needed to prevent seizure recurrence.
- If possible, propofol should be infused at a moderate-high rate (e.g. 50-80 mcg/kg/min). A low dose of vasopressor may be needed to allow for propofol administration. Phenylephrine*may be preferable here for patients without central access.
- For severely hypotensive patients, a midazolam infusion may be used instead of propofol. The main drawback of midazolam is that it accumulates and wears off slowly, delaying extubation.
*From PressorDex: Critical Care Medication Guide, 4th Edition. 2020, p x
-
-
- Phenylephrine
-
- Increased α1
- Increases SVR, Decreases CO at high doses
- Vasodilator Shock, Procedural hypotension
- 2-10 mcg/kg bolus then 1-5 mcg/kg/min
-
- Phenylephrine
-
For more details on the use of phenlyephrine, please see p 351 of the online pdf of the Wellington ICU Drug Manual, 2020.
super-refractory status epilepticus



