In this post I link to and excerpt from Dr Josh Farkas’ Internet Book of Critical Care [Link is to the TOC] Hyperosmolar hyperglycemic state (HHS) [Link is to the podcast and show notes] of July 31, 2020:
CONTENTS
- Pathophysiology
- Definition & diagnosis
- Evaluation
- Treatment
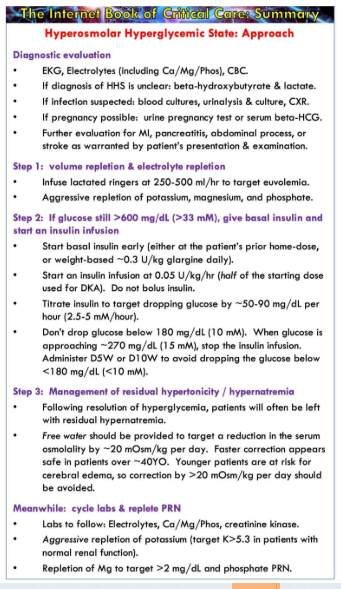
- Summary
- Podcast
- Questions & discussion
- Pitfalls
- PDF of this chapter (or create customized PDF)
summary
Pitfalls
- Hyperglycemia rarely causes mental status changes unless the serum osmolality is >320 mOsm. Thus, if the serum osmolality is <320 mOsm and mental status is significantly abnormal, look for an alternative explanation (Anna 2015).
- Patients with glucose >600 mg/dL (>33 mM) don’t necessarily have HHS, nor do they necessarily need an insulin infusion. Don’t assume that every patient with severe hyperglycemia requires ICU admission. As with everything in medicine, the context is king (what else is going on? does the patient appear sick or well?).
- True HHS develops slowly and should be corrected slowly. When in doubt, make small adjustments.
- The morbidity of HHS is due largely to underlying triggers, so search carefully for them (e.g., infection or infarction).
- Don’t forget to pay attention to sodium concentration and serum osmolality. Younger patients with HHS are at risk for cerebral edema if their tonicity is reduced too rapidly.
Going further:
- Hyperglycemic Hyperosmolar Syndrome (HHS) – emDocs by Anand Swaminathan
- IBCC chapter on hypernatremia