The following is from Episode 19 Part 2: Pediatric Gastroenteritis, Constipation and Bowel Obstruction from Emergency Medicine Cases:
PEDIATRIC CONSTIPATION
Definition as per Rome III criteria
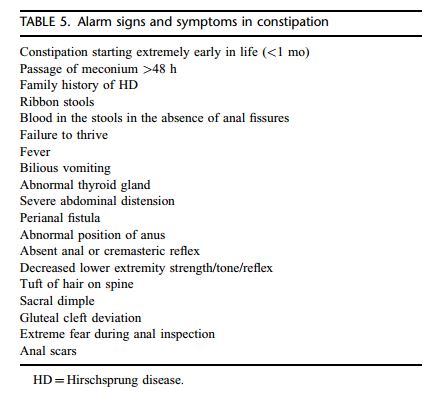
- [See Alarm Signs and Symptoms In Constipation below]
- ≤2 stools per week for a duration of 2mo if patient >2yo and for duration of 4mo if patient <2yo, or with evidence of overflow incontinence (no stool, then diarrhea, then no stool, etc), or stools that clog toilet
- Functional constipation is the most common cause of abdominal pain in children, but consider it a diagnosis of exclusion as severe underlying disease may be present
Differential diagnoses of Pediatric Constipation
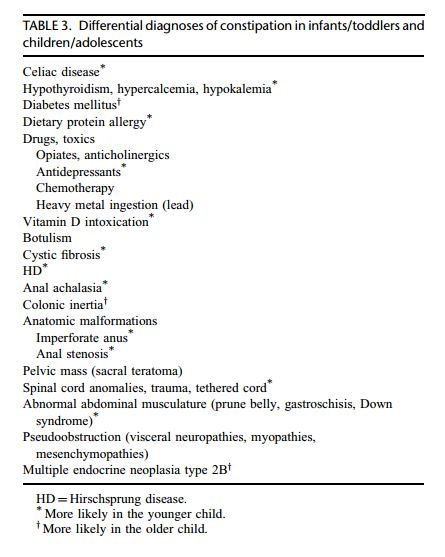
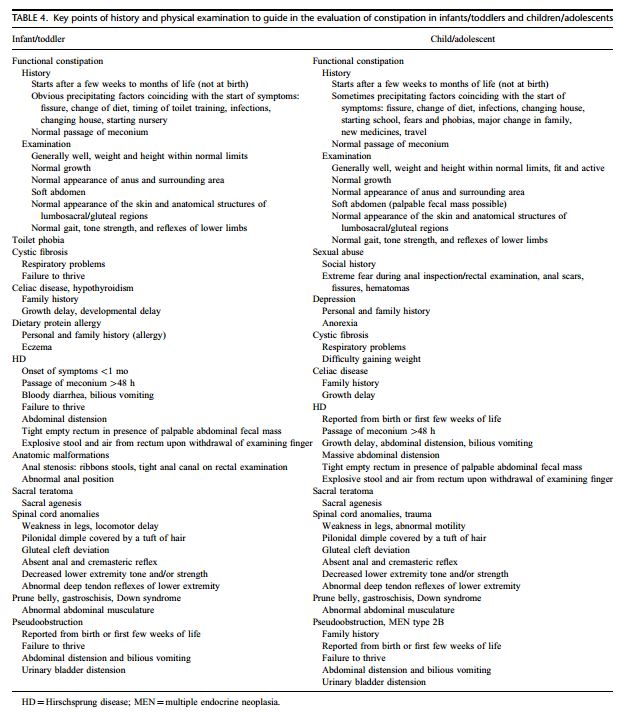
- [See Differential diagnosis in infants/toddlers and children/adolescents below]
- Hirschprung’s disease: severe obstipation with overflow diarrhea and abdominal distention in non‐ thriving and cranky child, which may present with toxic megacolon
- Cystic fibrosis and hypothyroidism: assess family history, and whether screening was performed
- Others: Down syndrome, myelomeningocele or neuromuscular problems (slow to walk, walking “funny”), celiac disease (family history), child abuse
Management
-
Oral medications work better when combined with enemas in the ER, but explain to the parents that it takes time to re‐train the bowel (sometimes years)
-
Enemas: if child <2yo, use saline enema 20cc/kg, and if child >20‐25kg, use adult fleet enema
-
At home: our experts prefer PEG 3350 (OTC Laxaday©) at dose of 1.5g/kg/d (rounded to the nearest ½cup of 17g) dissolved in 8ounces of juice, then titrate dose up or down for 1 soft stool per day, and with goal to slowly taper down
______________________________________________________________
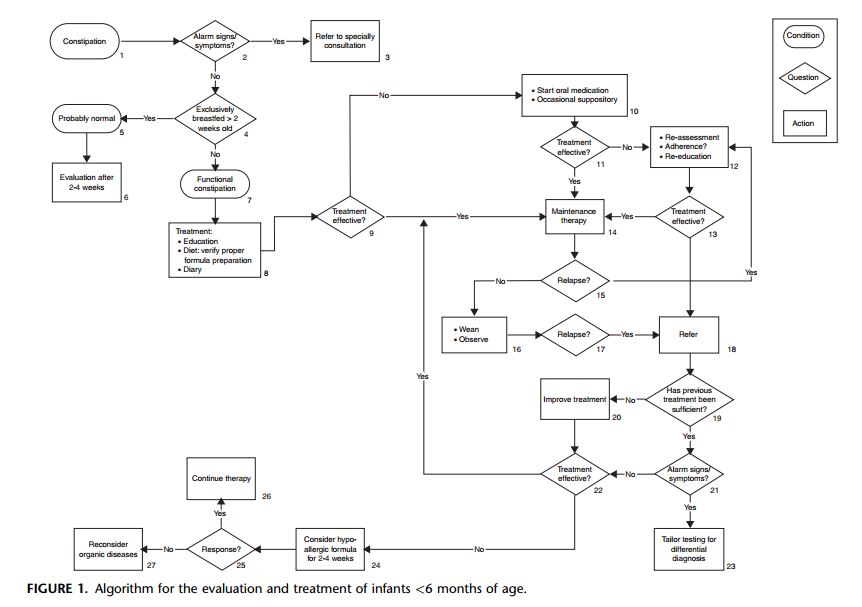
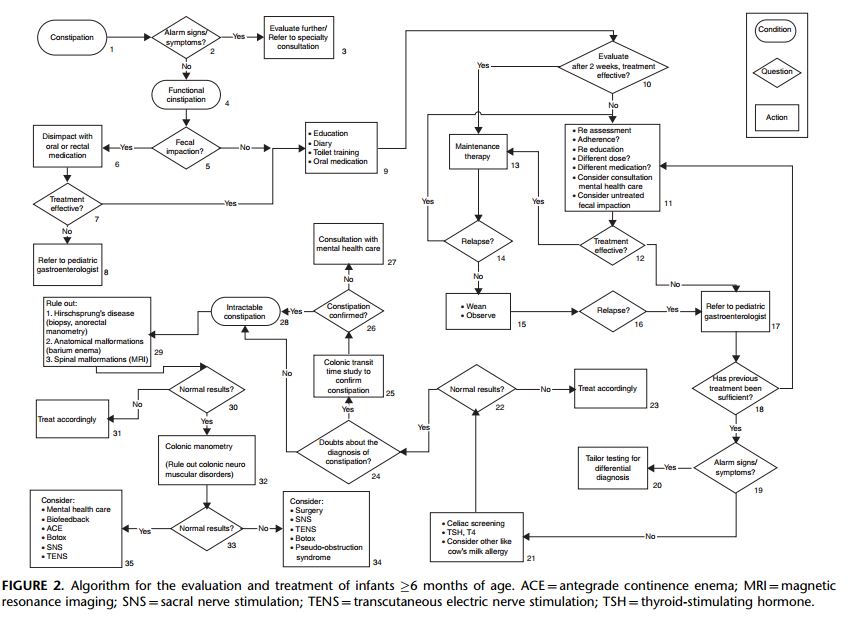
What follows is from the: Evaluation and Treatment of Functional Constipation in
Infants and Children: Evidence-Based Recommendations From ESPGHAN and NASPGHAN [PubMed Abstract] [Full Text PDF] J Pediatr Gastroenterol Nutr. 2014 Feb;58(2):258-74.