Note to myself and my readers: I only post excerpts from articles because doing so helps me remember the important points [spaced repetition]. Readers should download the complete article [links below] and review that.
In this post I link to and excerpt from Section 7 Screening for coronary artery disease in asymptomatic subjects from 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes: The Task Force for the diagnosis and management of chronic coronary syndromes of the European Society of Cardiology (ESC) [PubMed Abstract] [Full Text HTML] [Full Text PDF]. European Heart Journal, Volume 41, Issue 3, 14 January 2020, Pages 407–477.
Here are the links to the above guidelines:
Article Contents
All that follows is from Section 7 Screening for coronary artery disease in asymptomatic subjects.
In an effort to lower the high burden of coronary deaths in asymptomatic adults, numerous measurements of risk factors and risk markers, as well as stress tests, are often performed as screening investigations. The 2016 European Guidelines on CVD prevention in clinical practice* have focused on these issues in detail.15 These recommendations have been adapted for the purpose of these Guidelines.
*2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts)Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR) [PubMed Abstract]. Eur Heart J. 2016 Aug 1;37(29):2315-2381. doi: 10.1093/eurheartj/ehw106. Epub 2016 May 23.
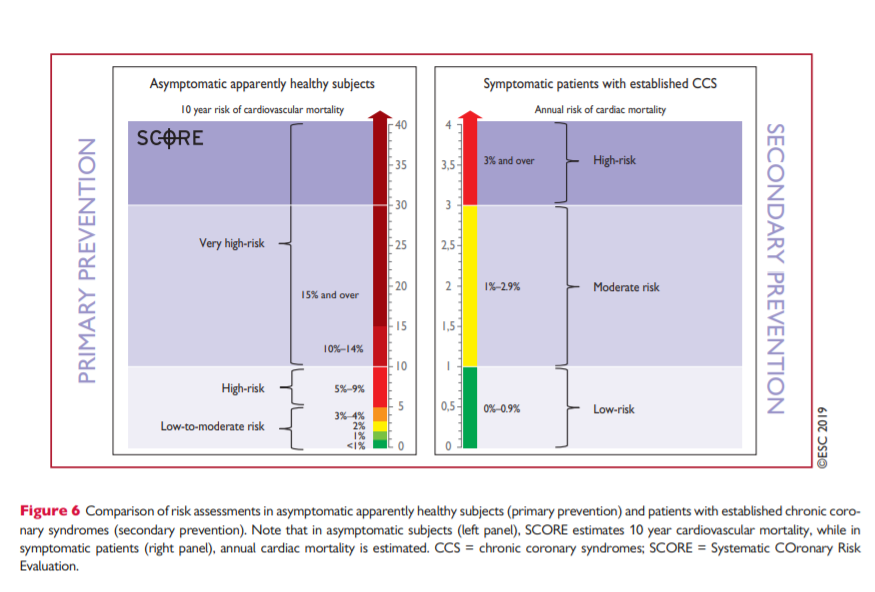
In general, the use of risk-estimation systems such as SCORE is recommended (see also Figure 6). Subjects with a family history of premature CAD should be screened for familial hypercholesterolaemia. Coronary calcium score, ankle−brachial index, and carotid ultrasound for plaque detection may provide useful information about the atherosclerotic risk in selected patients, but routine use of biomarkers or other imaging tests for CAD are not recommended. The new biomarkers have incremental predictive value over classical ones,448 but the net reclassification improvement is still only modest (7–18%) compared, for example, with the coronary calcium score, which has a net reclassification improvement of 66%.449
Only subjects at high event risk should be considered for further non-invasive or invasive testing. There are no data on how to manage asymptomatic subjects who receive testing and have a positive test result beyond the recommendations listed in these Guidelines. However, the principles of risk stratification, as described above for symptomatic patients, also apply to these individuals.450 It is important to remember that data demonstrating improved prognosis following appropriate management based on new biomarkers are still lacking.
It is important to note that patients with cancer and undergoing cancer treatment, or chronic inflammatory diseases such as inflammatory bowel diseases, rheumatoid arthritis, and systemic lupus erythematosus, may deserve more intensive risk screening, counselling, and management.451–454
Persons whose occupations involve public safety (e.g. airline pilots, or lorry or bus drivers), or who are professional or high-profile athletes, commonly undergo periodic testing for the assessment of exercise capacity and evaluation of possible heart disease, including CAD. Although there are insufficient data to justify this approach, these evaluations may be done for medicolegal reasons. The threshold for performing an imaging test in such persons may be lower than in the average patient. Otherwise, the same considerations as discussed above for other asymptomatic persons apply to these individuals.