5.7. Considerations for Restarting Anticoagulation
Should Anticoagulation be restarted?
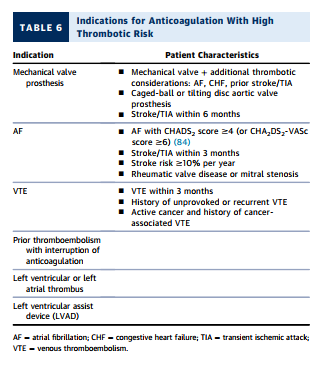
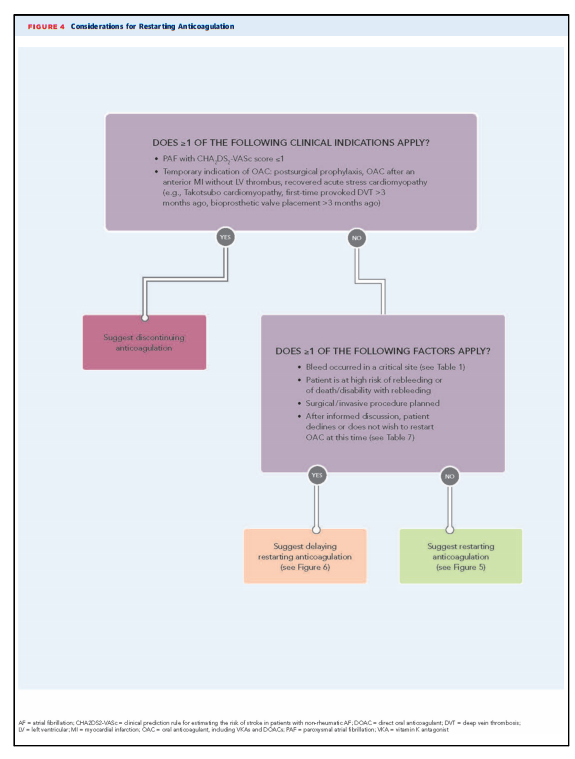
In most cases, there is net clinical benefit to restarting OAC after a bleeding event (85). After a patient has a bleeding event on OAC, the indication for OAC should be reassessed to determine whether continued therapy is warranted based on established clinical practice guidelines. The following are possible conditions for which OAC may no longer be indicated: n Paroxysmal atrial fibrillation with CHA2DS2-VASc score #1 n Temporary indication for OAC (e.g., postsurgical prophylaxis, OAC after an anterior myocardial infarction without left ventricular thrombus, recovered acute stress cardiomyopathy [e.g., Takotsubo cardiomyopathy], first time provoked venous thromboembolism >3 months ago, or bioprosthetic valve placement >3 months ago) (86)
If there is an ongoing indication for OAC, the clinician must evaluate the net clinical benefit of OAC in the context of a recent bleed to decide whether the risk of bleeding temporarily or permanently outweighs the benefit of treatment or thromboprophylaxis with OAC. This risk-benefit assessment should be conducted in consultation with other practitioners (e.g., surgeons, interventionalists, and neurologists) and in discussion with patients or caregivers