
This post features a link to and Resources from The ASCVD Risk Estimator Plus [Link is the Functioning Risk Estimator Plus app].
I originally posted this on Nov. 19, 2019. I reviewed and revised this post on 9-15-2020.
The following is from the above link:
For Optimal Use:
Estimate patient’s 10-year ASCVD risk at an initial visit to establish a reference point.
Forecast the potential impact of different interventions on patient risk.
Reassess ASCVD risk at follow-up visits. Follow up risk incorporates change in risk factor levels over time and requires both initial and follow up values.
Use the information above to help with clinician-patient discussions on risk and risk-lowering interventions. [This point refers to the three tabs at the very top of the app screen: Estimate Risk, Therapy Impact, and Advice Tab]
See the “About the App” screen * in this app for a definition of terms and additional instructions.
*What follows are excerpts from About the App screen
This app was last updated:
March 2019
Target patient population:
The Risk Estimator is intended for use in patients at risk for atherosclerotic coronary artery disease (ASCVD) and ASCVD-related events, especially due to dyslipidemia and hypertension.
The why and how of risk assessment*
When considering drug therapy for primary prevention of ASCVD, clinicians and patients should begin by calculating the 10-year and lifetime ASCVD risk estimates to identify patients in higher-risk groups who are likely to have greater net benefit and lower number needed to treat for both statins and antihypertensive therapy. Current U.S. prevention guidelines for blood pressure and cholesterol management recommend use of the pooled cohort equations (PCE) to assess 10-year ASCVD risk and start a process of shared decision-making between clinicians and patients. Lifetime risk assessment appears to be particularly useful for describing and communicating ASCVD risk in younger individuals. The Million Hearts Longitudinal ASCVD Risk Assessment equation can also be used to update a patient’s risk by comparing change in risk factors from a previous to the current visit. (See “Terms and Concepts” in the Resources section for more information about each of these calculations and where they are utilized in the app.)
The guidelines recommend the use of the PCE as an important starting point, but not as the final arbiter, for decision-making in primary prevention of ASCVD. The initial risk estimate should form the basis for a discussion that includes:
- Burden and severity of CVD risk factors and control of these risk factors.
- Presence of risk-enhancing conditions (See “ASCVD Risk Enhancing Factors” in the Resources section at the bottom of this app). It is difficult to determine how much a risk-enhancing factor may change a patient’s 10-year risk estimate quantitatively and therefore, clinician judgment is also crucial to determine whether factors are significant enough to reclassify an individual’s risk category.
- Adherence to healthy lifestyle recommendations. For all patients, appropriate lifestyle modification should be recommended. In patients at higher absolute predicted risk for ASCVD (typically, a 10-year estimated risk) more intensive lifestyle efforts are recommended.
- – Potential for ASCVD risk-reduction benefits from statins and antihypertensive drug therapy, and the potential for adverse effects and drug–drug interactions. The Million Hearts Longitudinal ASCVD Risk Assessment equations can also help to quantify potential benefits of preventive therapies based on high-quality evidence, and can be accessed in the Therapy Impact tab at the top of this app.
- Patient preferences regarding the use of medications for primary prevention. In addition, in patients at intermediate 10-year risk (7.5% to <20%), and select patients at borderline risk (5% to <7.5%) for whom, after the clinician-patient discussion, the benefits of statin medication for the individual patient remain unclear, the patient has important risk-modifying factors that suggest a better or worse risk than the original estimate, or if the patient is undecided regarding drug therapy, additional testing to help with the decision making is reasonable. In such cases, additional testing should only be used if it can provide sufficient information to modify the decision. Presently, the best additional test to help reclassify ASCVD risk in these situations is measurement of a CAC score for decision-making regarding statin therapy.* Please see “Using A CAC Score to Inform Decision Making” in the Resources section at the bottom of this app for more information.
*But for a thoughtful opposing view please see The Case Against Coronary Artery Calcium Scoring for Cardiovascular Disease Risk Assessment [PubMed Abstract] [Full Text HTML] [Full Text PDF].
Most cardiovascular experts now favor use of the Coronary Artery Calcium Score if the clinician and/or patient want more risk stratification beyond the Pooled Cohort Equations.
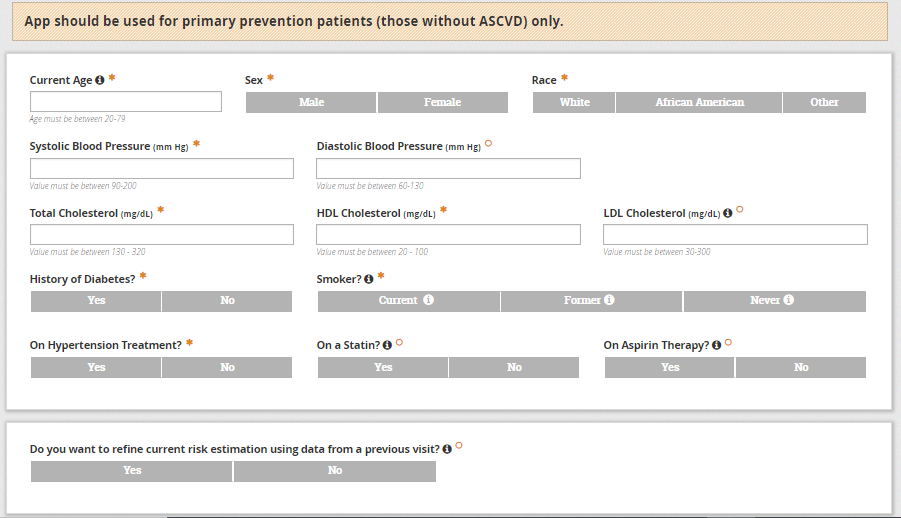
What follows below is a non-functioning picture of the app.
App should be used for primary prevention patients (those without ASCVD) only.

And here is a link to About The App: which has information on:
- The why and how of risk assessment*
- How to use this app for risk assessment
For more information about the inputs and calculations used in this app, see “Terms and Concepts” in the Resources tab below.
**10-year risk for ASCVD is categorized as:
Low-risk (<5%)
Borderline risk (5% to 7.4%)
Intermediate risk (7.5% to 19.9%)
High risk (≥20%)
*Indicates a field required to calculate current 10-year ASCVD risk for patients age 40-79. Risk will automatically calculate once these fields are populated.
oIndicates additional questions required to determine individualized patient advice for patients age 40-79. Answering these questions in addition to the indicated risk fields will activate the Therapy Impact and Advice tabs.



