
The following are excerpts from Screening for Endocrine Hypertension: An Endocrine Society Scientific Statement [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Endocrine Reviews, Volume 38, Issue 2, 1 April 2017, Pages 103–122:
I. Introduction
Hypertension affects 28.6% of adults in United States
(1–3). In most, hypertension is primary (essential or
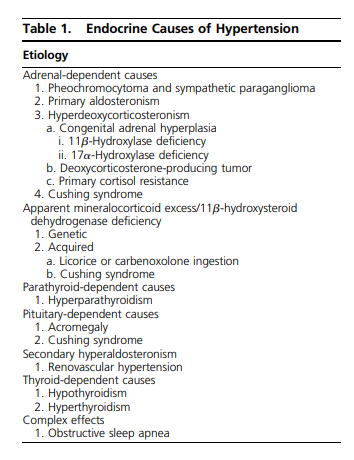
idiopathic), but a subgroup of approximately 15% has secondary hypertension (4, 5). More than 50% of children who present with hypertension have a secondary cause (6). In young adults (,40 years old), the prevalence of secondary hypertension is approximately 30% (7). The secondary causes of hypertension include renal causes (e.g., renal parenchymal disease) and endocrine causes. Hypertension may be the initial clinical presentation for at least 15 endocrine disorders (Table 1). An accurate diagnosis of endocrine hypertension provides clinicians with the opportunity to render a surgical cure
or to achieve an optimal clinical response with specific
pharmacologic therapy (8). Primary aldosteronism (PA)
is a disorder that clinicians should consider in most patients with hypertension (9). Herein, we review the different forms of endocrine hypertension with a focus on prevalence, clinical presentation, guidance on when to perform case-detection testing, and currently available case detection tests (Fig. 1).

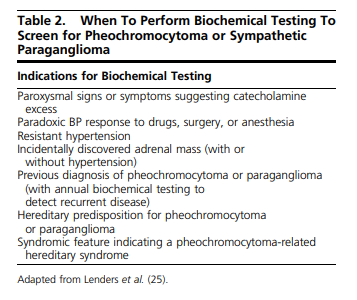
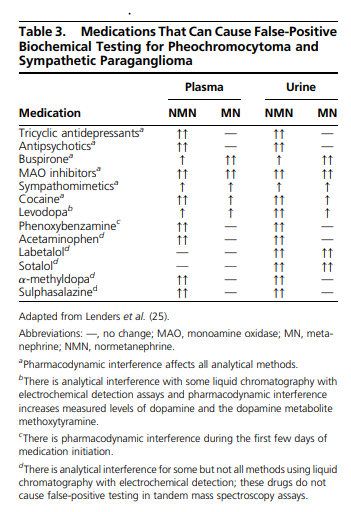
II. Pheochromocytoma and Paraganglioma
III. Primary Aldosteronism
In PA, aldosterone production exceeds the body’s requirements and is relatively unchecked by its normal regulator, the renin-angiotensin II system (37, 38). Excessive unregulated production of aldosterone results in increased sodium reabsorption via amiloride-sensitive epithelial sodium channels within the distal nephron, leading to hypertension and renin-angiotensin II suppression. Urinary loss of potassium and hydrogen ions, exchanged for sodium at the distal nephron, may result in hypokalemia and metabolic alkalosis (37, 38).
A. Prevalence
Once thought to be a rare condition and not worth
investigating in patients with hypertension unless hypokalemic, PA is now considered the most common, specifically treatable, and potentially curable form of
hypertension, accounting for at least 5% to 10% of
hypertensive patients, with most patients normokalemic
(39, 40). In resistant hypertensive cohorts, the prevalence
of PA is approximately 20% (41, 42). Most patients with
PA are diagnosed during their third to sixth decades (43).C. Who should be screened?
Clinicians should consider PA screening for most patients with hypertension. In part, this is because hypertension in PA responds well to specific treatments directed against aldosterone excess. Unilateral laparoscopic adrenalectomy in patients with unilateral forms of PA cures hypertension in 50% to 60% of cases and results in significant improvements in the remainder (58–60). For nonoperated patients, medications that antagonize aldosterone action (e.g., spironolactone, eplerenone, and amiloride) lead to substantial and often marked improvements in hypertension control (61, 62).
The Endocrine Society clinical practice guideline on
PA recommends the case detection of PA in patient
groups with relatively high prevalence of PA (9). These
include the following: patients with a sustained elevated
BP [BP $150 mm Hg (systolic) and/or 100 mm Hg
(diastolic)]; hypertension (BP .140/90 mm Hg) resistant
to three conventional antihypertensive drugs, including a
diuretic; controlled BP (BP ,140/90 mm Hg) with four or
more antihypertensive drugs; hypertension and spontaneous or diuretic-induced hypokalemia; hypertension
and adrenal incidentaloma; hypertension and OSA; or
hypertension and a family history of early-onset hypertension or cerebrovascular accident at a young age (,40
years old). Given the known existence of familial forms,
the guideline also recommends case detection for all
hypertensive first-degree relatives of patients with PA (9).The aldosterone/renin ratio
The aldosterone/renin ratio (ARR) is the most reliable
available screening test; it is more specific than renin
measurement (levels of which are almost always suppressed in patients with PA) and more sensitive than
plasma potassium or aldosterone measurements. The
ratio becomes elevated before aldosterone or plasma
potassium leave their normal ranges (52).IV. Other Forms of Mineralocorticoid Excess
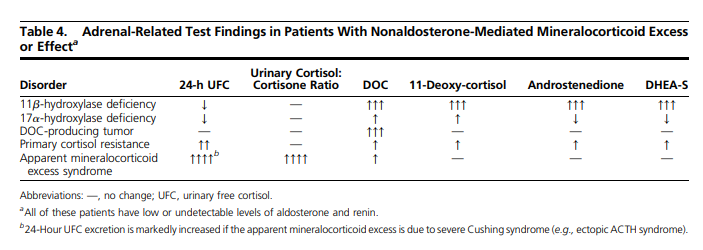
or EffectTable 1 lists medical disorders associated with mineralocorticoid excess resulting from deoxycorticosterone (DOC) or cortisol. Clinicians should consider these disorders if blood levels of aldosterone and renin are low in a patient with hypertension and hypokalemia (81).
V. Secondary Aldosteronism and Renovascular Hypertension
Most studies addressing the prevalence of renovascular
disease focus on the frequency of identifying renal artery
stenosis rather than establishing the actual occurrence of
hypertension. This distinction is important because the
kidney tolerates some degree of vascular occlusion without
clinical manifestations. The prevalence of actual RVH is
substantially less than that for renal artery stenosis. Some
argue that establishing a diagnosis of RVH depends on
reducing BP after technically successful revascularization
or removal of the affected kidney.Most renal artery stenosis in the United States is caused
by atherosclerotic disease (85%) or some form of
fibromuscular dysplasia (15%). The prevalence of
atherosclerotic renal artery stenosis increases with age
and other atherosclerotic manifestations. Population based studies indicate that 6.8% of individuals older than 65 years have renal artery stenosis with more than
60% lumen occlusion.Studies of image-based screening in patients undergoing angiography for other atherosclerotic diseases
showed that 14% to 33% of these patients have renal
artery stenosis, depending upon the extent of disease.
Similarly, studies of image-based screening in potential
kidney donors showed that 3% to 5% of normal subjects
have some degree of fibromuscular dysplasia.
How often these lesions produce RVH and the true
prevalence of RVH remain unclear, but estimates from
referral hypertension centers suggest that 1% to 5% of
hypertensive subjects may have a component of RVH.C. Who should be screened?
The utility of screening and diagnostic testing for RVH
and other causes of secondary aldosteronism partly depends
upon the commitment to act upon the results. The pressure
to identify renal artery stenosis has diminished in recent
years. One reason for this is that medical therapy is remarkably effective at blocking the RAAS, without the need
for either endovascular or surgical revascularization. Several
recent prospective randomized controlled trials (RCTs) have
failed to identify major additional benefits from stent revascularization for atherosclerotic renal artery stenosis (98).
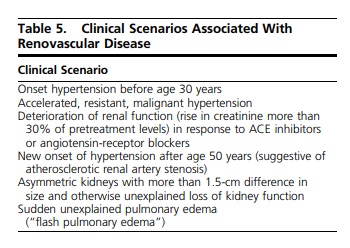
Thus, it may be argued that clinicians should limit screening
for these disorders to cases where medical therapy is failing
or the risks of circulatory or renal failure truly warrant restoring the circulation, as identified in Table 5. Because these
RCTs failed to enroll or excluded many high-risk subjects,
clinicians must individualize treatment of many patients,
particularly those with rapidly declining kidney function,
accelerated hypertension, or episodes of pulmonary edema.
VI. Other Endocrine Disorders Associated With Hypertension
A. Cushing syndrome
Prevalence
Iatrogenic Cushing syndrome is relatively common.
However, endogenous Cushing syndrome is rare, with an incidence of less than one per 1 million people per year
(103). Excess ACTH secretion by a pituitary tumor is the
cause of endogenous Cushing syndrome in 85% of patients and is termed “Cushing disease.” Cushing disease
occurs five times more frequently in women than in men,
with the peak incidence occurring between 20 and 50
years of age. Ectopic ACTH-secreting neoplasms and the
ACTH-independent forms of Cushing syndrome (e.g.,
adrenal adenoma, adrenal carcinomas, and adrenal
nodular hyperplasias) are responsible for 15% of the
endogenous cases. Hypertension occurs in 75% to 80%
of patients with Cushing syndrome (104, 105). The
mechanisms of hypertension include increased production of DOC, enhanced pressor sensitivity to endogenous vasoconstrictors (e.g., epinephrine, angiotensin
II), increased cardiac output, activation of the RAAS by
increased hepatic production of angiotensinogen, and
cortisol activation of the mineralocorticoid receptor.The case-detection tests for endogenous cortisol excess
include a 1-mg overnight dexamethasone-suppression
test and measuring midnight salivary cortisol and free
cortisol in a 24-hour urine collection. When results of
case-detection tests for Cushing syndrome are abnormal,
clinicians should pursue confirmatory testing. The Endocrine Society’s clinical practice guideline on Cushing
syndrome further details tests that confirm Cushing
syndrome and determine the cause of cortisol excess (95).B. Thyroid dysfunction
C. Hypercalcemia and primary hyperparathyroidism
D. Acromegaly
E. Obstructive sleep apnea
VII. Summary of Overall Approach to Considering and Detecting Endocrine Hypertension
Clinical context is important. For example, case detection
for endocrine hypertension may not be clinically important
in an older patient with multiple life-limiting comorbidities. However, screening for endocrine hypertension may
be key to enhancing and prolonging life in most patients
with hypertension, especially younger patients.A. Case in point
A 36-year-old woman presents with new-onset hypertension with repeated measurements of a systolic BP of
150 to 170 mm Hg and a diastolic BP of 95 to 110 mm
Hg. Except for occasional headaches and palpitations,
she is asymptomatic. She has been healthy and active. She
does not use tobacco or alcohol. She has gained 5 kg over
the past 1 year, and she has a history of recurrent renal
lithiasis. Her husband said that she snores at night, but he
has not observed periods of apnea. On questioning, she
said that she does not feel rested in the morning. When she
was in her 30s, she was told that she had a goiter. Her first
menstrual period was at age 11 years and she has three
biologic children. She does not eat confectionary licorice.
Her family history is positive for hypertension in her
father, hyperthyroidism in her maternal grandmother,
and hypothyroidism in her mother. There is no family
history of endocrine disorders or adrenal tumors.
The degree of hypertension in this 36-year-old woman
merits an investigation for secondary causes. Because of
the history of headaches and palpitations, case-detection
testing for pheochromocytoma is indicated. We should
check serum calcium and phosphorus levels because of
her history of renal lithiasis. The weight gain over the past
year could be a clue to Cushing syndrome and we should
exclude this diagnosis. Her history of snoring and not
feeling rested in the morning should prompt testing for
OSA. We should exclude thyroid dysfunction based on
her history of a goiter and family history of autoimmune
thyroid disease. Because there are usually no symptoms
or signs of PA, we should exclude this diagnosis in all
patients with marked hypertension. In addition, she is in
the age group in which we should consider fibromuscular
dysplasia of the renal arteries. Depending on the degree of
hypertension and urgency, we can perform case-detection
testing for the potential diagnoses listed here either sequentially or simultaneously.



