
Note to myself and my readers: I strongly suggest that instead of today’s show notes below, you review CDC Pocket Guide (includes management protocol): https://www.cdc.gov/dengue/hcp/pocketguide/index.html
I have posted the above pocket guide at Linking To And Embedding The CDC’s Pocket Guide To Dengue Fever Management
Posted on May 6, 2025 by Tom Wade MD
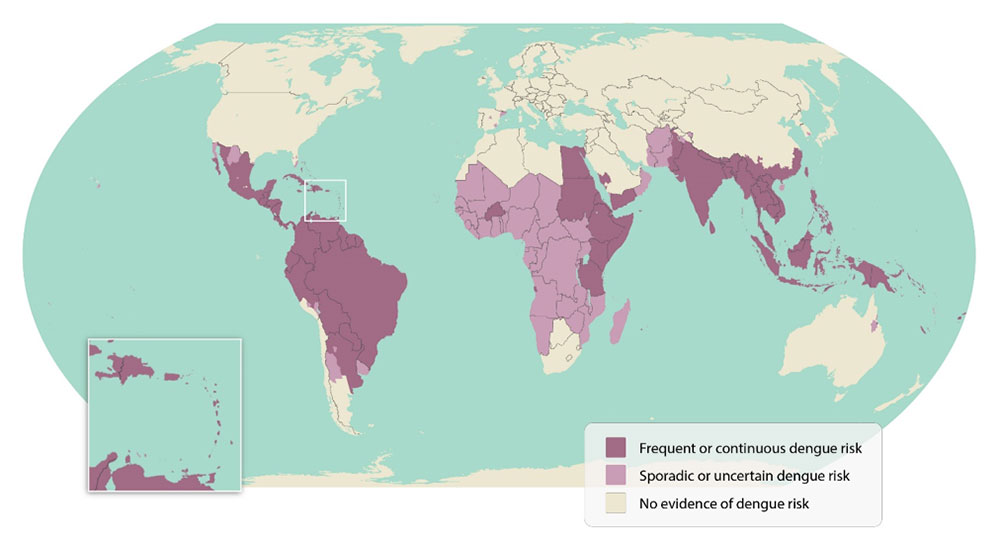
In addition to today’s resource below, please see the CDC‘s Areas with Risk of Dengue:
Key points
- Almost half of the world’s population, about 4 billion people, live in areas with a risk of dengue.
- Anyone who lives in or travels to an area with risk of dengue is at risk for infection.
- Before you travel, find country-specific travel information to help you plan and pack.
World map highlighting areas of dengue risk.
Today I review EM Quick Hits 63‘s* “Recognition and management of dengue fever”.
*Helman, A. Freedman, S. Morgenstern, J. McArther, M. Petrosoniak, A. Long, B. Gotlieb, M. EM Quick Hits 63 – S-TEC and HUS, IM Epinephrine in OHCA, Dengue, Geriatric Trauma Imaging, TTP. Emergency Medicine Cases. March, 2025. https://emergencymedicinecases.com/em-quick-hits-march-2025/. Accessed May 4, 2025.
All that follows is from the above resource.
Matthew McArther on recognition and ED management of dengue fever (33:56)
Recognition and management of dengue fever
Podcast: Play in new window | Download (Duration: 1:06:46 — 61.2MB)
Background: Dengue is a mosquito-borne flavivirus (related to Zika and West Nile) which transmits between humans by mosquitos and is endemic to many countries in tropical and subtropical regions. It has been an increasing public health concern due to increasing outbreaks over the last decade. All 4 types of Dengue cause acute infections in humans but are not known to cause chronic infections.
75% of dengue infections are asymptomatic. However, 2-5% of dengue can progress to severe dengue.
There are 3 phases of dengue:
- Febrile phase (2-7 days): Rapid onset of high fever, headache, joint pain, eye pain, myalgia, nausea, vomiting, and a macular or maculopapular rash
- Minor bleeding and petechiae can be elicited by the tourniquet test (inflation to halfway between SBP and DBP x5 min, +ve test if >10 new petechiae appear in a 1 square inch of skin within 1-2 min of cuff deflation)
- Blood work may show leukopenia, thrombocytopenia, and mild liver enzyme elevation
- Confirmatory test for dengue: Viral molecular testing and IgM levels (positive within 4-7 days of infection
- Critical phase (severe cases only): Plasma leakage leading to shock, bleeding, and organ dysfunction
- Treatment: IV fluid resuscitation and supportive care
- Risk factors for developing into severe dengue include extremes of age, immunosuppression, baseline comorbidities, and previous dengue infection
- Recovery phase: Resolution of plasma leakage and hemorrhage. Reabsorption of extravasated fluids
- Some may develop further rashes or severe post-viral fatigue lasting days to weeks
The updated WHO classification system for dengue includes dengue, dengue with warning signs, or severe dengue. Consider the diagnosis of dengue in patients coming from an endemic area who have fever and any 2 of: aches, rash, nausea, vomiting, leukopenia, and positive tourniquet test.
Warning signs for severe dengue:
- Intense, continuous abdominal pain or tenderness
- Persistent vomiting
- Fluid accumulation (e.g. ascities, pleural effusion)
- Mucosal bleeding
- Altered mental status
- Hepatomegaly
- Rapidly rising hematocrit (in measures six hours apart)
Severe dengue = shock, clinically significant bleeding, or severe organ impairment
There are no specific therapies or vaccines for Dengue. Management is primarily supportive:
- Mild cases without warning signs: Outpatient management with close follow up, oral hydration, and tylenol for fever
- Avoid NSAIDs and steroids (increased risk of GI bleed)
- Patients with risk factors (e.g. age, comorbidities): consider admission for close observation
- Patients with warning signs: admission and IV fluid resuscitation with isotonic fluids (10mL/kg over 1 hour) followed by reassessment and gradual tapering of IV fluids
- Severe dengue: ICU level care with large volume resuscitation (consider IV colloids if not responsive to aggressive crystalloids).
- Prophylactic platelet transfusion is not recommended
Bottom line: Dengue is self-limiting in most cases but can be life-threatening in 2-5% of patients. Management of dengue is primarily supportive with oral or IV fluid resuscitation.
References
- CDC Pocket Guide (includes management protocol): https://www.cdc.gov/dengue/hcp/pocketguide/index.html
- Adams LE, Wong JM, Paz-Bailey G. Dengue. JAMA. 2024 Dec 24;332(24):2109-2110. doi: 10.1001/jama.2024.21094. PMID: 39602174.
- Paz-Bailey G, Adams LE, Deen J, Anderson KB, Katzelnick LC. Dengue. Lancet. 2024 Feb 17;403(10427):667-682. doi: 10.1016/S0140-6736(23)02576-X. Epub 2024 Jan 24. PMID: 38280388.
- Bhatt S, Gething PW, Brady OJ, Messina JP, Farlow AW, Moyes CL, Drake JM, Brownstein JS, Hoen AG, Sankoh O, Myers MF, George DB, Jaenisch T, Wint GR, Simmons CP, Scott TW, Farrar JJ, Hay SI. The global distribution and burden of dengue. Nature. 2013 Apr 25;496(7446):504-7. doi: 10.1038/nature12060. Epub 2013 Apr 7. PMID: 23563266; PMCID: PMC3651993.



