
Here are the links to Dr. Josh Farkas’ outstanding podcast and show notes on Angioedema: Internet Book Of Critical Care [This link is to the Table of Contents] chapter & cast – [Bradykinin-Induced] Angioedema. August 1, 2019 by Josh Farkas:
Here are excerpts from Dr. Farkas excellent post [Note to myself: review complete post, excerpts are just to help place the post in my mind.]:
CONTENTS
- Overview
- Histamine-mediated angioedema
- Bradykinin-mediated angioedema
- Extubating the angioedema patient
- Algorithms
- Podcast
- Questions & discussion
- Pitfalls
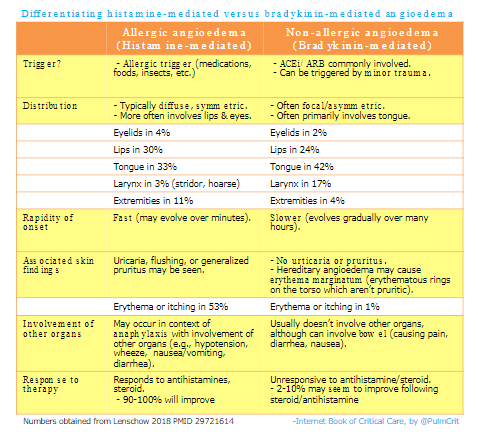
clinical characteristics of histamine-mediated versus bradykinin-mediated angioedema.
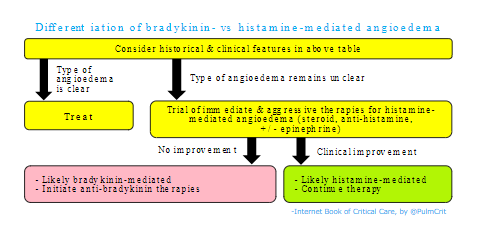
approach to sorting out the etiology of angioedema
- Clearly differentiating the cause of angioedema is important (because the treatments are entirely different).
- Histamine-mediated angioedema will almost always respond rapidly to aggressive treatment (with antihistamine, steroid, and possibly epinephrine). In contrast, bradykinin-mediated angioedema won’t respond to these treatments (and tends to progress slowly, over a period of hours). Therefore, an immediate therapeutic trial of therapies for histamine-mediated angioedema can be used as a diagnostic/therapeutic approach to undifferentiated angioedema (29721614).
Potential Indications For Intubation [in Angioedema]
- (1) Stridor, dyspnea
- (2) Inability to handle secretions
- (3) Progressive deterioration of edema (intubation may become more difficult over time if edema worsens)
- (4) Nasolaryngoscopy shows significant laryngeal edema or impending closure of the posterior pharynx. When in doubt, nasolaryngoscopy may help reveal whether there is significant laryngeal edema. The true threat to the airway is the larynx and posterior tongue – not the lips and anterior tongue.
Intubation is fraught with hazard
- Airway manipulation may worsen swelling.
- Laryngeal edema will often preclude the use of a laryngeal mask airway.
- In severe angioedema, orotracheal intubation may simply be impossible.
scenario #1: the crashing angioedema patient (extremely rare)
- Description
- Patient is at immediate risk of losing their airway.
- Patient is stridulous, sitting bolt upright, and struggling for breath.
- Patient may be unable to lie down.
- Potential management: Ketamine-dissociated cricothyrotomy
- Place the patient on 100% FiO2 using one of the following:
- i) High-flow nasal cannula at 100% FiO2 and 60 liters flow
- ii) BiPAP mask
- iii) 100% Non-rebreather facemask set to flush rate (crank the flow rate well past the 15 liters/min mark)
- iv) 100% non-rebreather facemask set to 15 liters/minute plus a nasal cannula underneath it running at 15 liters/minute
- Provide a dissociative dose of IV ketamine (e.g. 1.5-2 mg/kg) slowly over ~120 seconds. This should fully dissociate the patient, without impairing the respiratory drive. Patients with a history of alcoholism may require more ketamine to fully dissociate.
- Perform a scalpel-finger-bougie cricothyrotomy. The patient should continue breathing throughout the entire procedure, so you should be able to take your time a bit with this. However, if asphyxiation occurs, the procedure should be achievable very rapidly.
scenario #2: the non-crashing angioedema patient
- Description
- The patient requires intubation, but isn’t actively crashing.
- There is time to call for help and additional equipment.
- Suggested management: The awake double setup:
- Obtain an experienced intubator and someone competent at scalpel-finger-bougie cricothyrotomy (Note: it doesn’t matter whether this person is a surgeon, what matters is skill in this specific procedure).
- Perform awake fiberoptic intubation. These patients often have tongue swelling, so the best approach is often nasotracheal intubation (for taller patients, consider obtaining an extra-long ETT for nasotracheal intubation).
- During the intubation procedure, the second operator should be prepared to perform cricothyrotomy if the airway is lost.
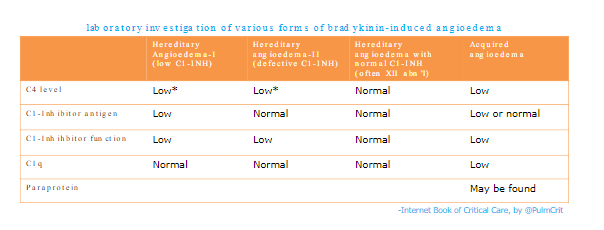
Diagnosis Of Bradykinin Angioedema
Labs won’t return fast enough to affect management, but should be considered to guide future management. Administration of some therapies (e.g. fresh frozen plasma, C1-inhibitor concentrate) may impair the accuracy of subsequent laboratory values.
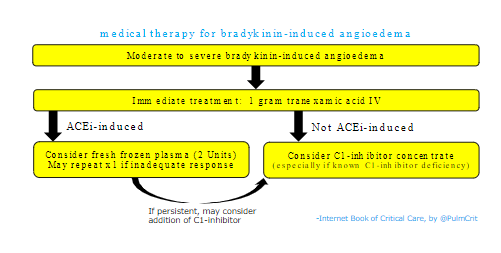
Start at Tranexamic Acid
Additional Resources:
(1) Awake Cricothyrotomy: A Novel Approach to the Surgical Airway in the Tactical Setting [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Wilderness & Environmental Medicine. 2017 Jun;28(2S):S61-S68. doi: 10.1016/j.wem.2017.02.003.
(2) PHARM Podcast 173 Awake Cricothyrotomy: A Novel Approach to the Surgical Airway in the Tactical Setting by Dr. Minh LeCong of PHARM: Prehospital & Retrieval Medicine.



