
In this post, I link to and excerpt from Clinical characterization of dysautonomia in long COVID-19 patients [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. Published: 07 July 2021. Nature Scientific Reports.
All that follows is from the above article.
Abstract
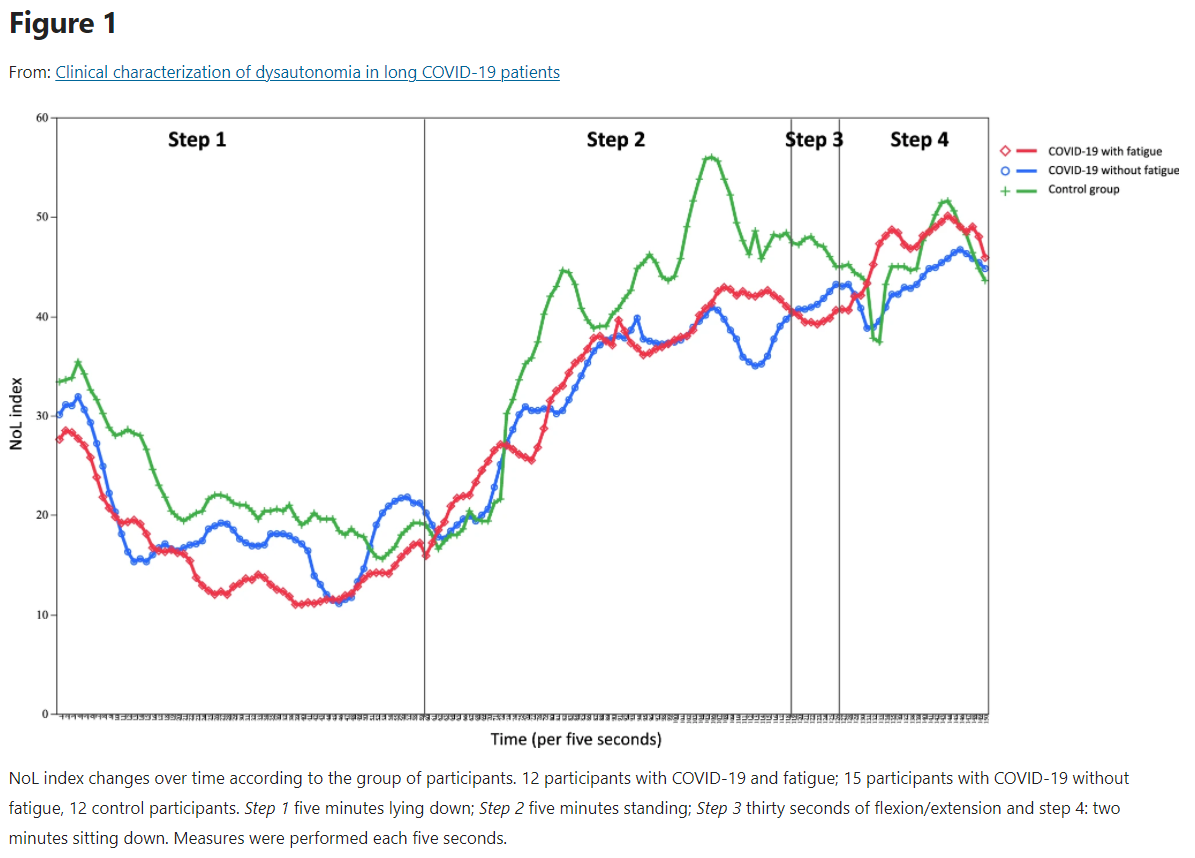
Increasing numbers of COVID-19 patients, continue to experience symptoms months after recovering from mild cases of COVID-19. Amongst these symptoms, several are related to neurological manifestations, including fatigue, anosmia, hypogeusia, headaches and hypoxia. However, the involvement of the autonomic nervous system, expressed by a dysautonomia, which can aggregate all these neurological symptoms has not been prominently reported. Here, we hypothesize that dysautonomia, could occur in secondary COVID-19 infection, also referred to as “long COVID” infection. 39 participants were included from December 2020 to January 2021 for assessment by the Department of physical medicine to enhance their physical capabilities: 12 participants with COVID-19 diagnosis and fatigue, 15 participants with COVID-19 diagnosis without fatigue and 12 control participants without COVID-19 diagnosis and without fatigue. Heart rate variability (HRV) during a change in position is commonly measured to diagnose autonomic dysregulation. In this cohort, to reflect HRV, parasympathetic/sympathetic balance was estimated using the NOL index, a multiparameter artificial intelligence-driven index calculated from extracted physiological signals by the PMD-200 pain monitoring system. Repeated-measures mixed-models testing group effect were performed to analyze NOL index changes over time between groups. A significant NOL index dissociation over time between long COVID-19 participants with fatigue and control participants was observed (p = 0.046). A trend towards significant NOL index dissociation over time was observed between long COVID-19 participants without fatigue and control participants (p = 0.109). No difference over time was observed between the two groups of long COVID-19 participants (p = 0.904). Long COVID-19 participants with fatigue may exhibit a dysautonomia characterized by dysregulation of the HRV, that is reflected by the NOL index measurements, compared to control participants. Dysautonomia may explain the persistent symptoms observed in long COVID-19 patients, such as fatigue and hypoxia.
Introduction
Increased numbers of COVID-19 patients, continue to experience symptoms several months after mild cases of COVID-191. Reported symptoms lead to disability with debilitating fatigue, breathlessness, headaches, muscle and/or joint pain, brain fog, memory loss, sensation of pressure on the chest, palpitations, nausea, dramatic mood swings in combination with exercise intolerance and a relapsing–remitting pattern of recurrence2. Among these symptoms, several are related to neurological manifestations, including fatigue, anosmia, hypogeusia, and headaches3, and also respiratory symptoms, such as hypoxia4. Nevertheless, the involvement of the autonomic nervous system (ANS) which can aggregate all these neurological symptoms in COVID-19 infection has been under reported in the literature5. One of the last and recent hypotheses is that these symptoms could be the manifestation of a dysautonomia in long COVID-19 infection6.
Dysautonomia is marked by the failure or the increased of the sympathetic or parasympathetic components activities in the ANS. Dysautonomia shows numerous clinical symptoms, such as fatigue, labile blood pressure, orthostatic hypotension, dysfunction in heart rate variability (HRV), apparition of impotence, dysfunction of bladder, and damages in bowel functions. Dysautonomia could be acute or chronic, progressive but also reversible and was associated with numerous pathologies, such as alcoholism, diabetes, or either Parkinson’s disease. Dysautonomia was also associated with viral infections, including hepatitis C virus, HIV, or Epstein-Barr virus5. Fatigue is one of the major clinical characteristic of dysautonomia in COVID-19 patients7,8,9.
HRV measurement is a commonly used method for cardiovascular follow-up in healthy participants, athletes and cardiovascular patients10. HRV is mainly related to emotional, social, cognitive and health levels11. HRV is the main marker of the modulation of the sympathetic and parasympathetic branches of the ANS, and thus, of dysautonomia12. The low-frequency band reflects the modulation of sympathetic and parasympathetic branches on the heart13 and has been considered as an index of the sympathovagal imbalance14. In the current study, we apply the nociception level (NOL) index to estimate HRV and overall ANS balance. The NOL algorithm (Medasense Biometrics, Ramat Gan Israel)* is a multiparameter nonlinear combination of HR, HRV, amplitude of the finger photoplethysmogram, skin conductance level, and their time derivatives, obtained using a non-invasive finger probe, displayed on the monitor screen as a scale of 0–100 derived using a random forest regression15.
*Introducing the NOL® (Nociception Level) Index Algorithm: A Technical Overview. © Copyright, 2020, Medasense Biometrics Ltd. All rights reserved. | MK2U-02-438 R03
Here, we hypothesize that dysautonomia could occur in secondary COVID-19 infection, also called “long COVID” infection. We aim to demonstrate this phenomenon by illustrating HRV dysregulation, reflected through the NOL index showing the sympathetic/parasympathetic balance, in long COVID-19 participants. We propose that the symptoms secondary to COVID-19 could be directly related to this virus or its immune-related dysregulation to the ANS, leading to transient or long-term dysautonomia.
Methods
The present study prospectively included 39 participants from December 2020 to January 2021: 12 participants with COVID-19 diagnosis and fatigue, 15 participants with COVID-19 diagnosis without fatigue and 12 control participants without COVID-19 diagnosis and without fatigue. COVID-19 diagnosis was defined as positive polymerase chain reaction (PCR) test, serologic test or computed tomography (CT) scan. Participant’s eligibility for inclusion in the study was assessed during their long COVID-19 follow-up in the Department of physical medicine and rehabilitation of the Foch hospital (Suresnes, France). This follow-up aims to enhance the participants in physical activity through a personalized program of exercises-long COVID-19 rehabilitation. Exclusion criteria were age inferior to 18 years, Nociception level unusable, vasoactive medication, toxicological or alcoholic participants, BMI superior to 35, previous intensive care unit (ICU) hospitalization and participants legally protected or deprived of their freedom.
HRV was reflected using the NOL index, initially developed in the operating theater to guide analgesia administration during surgery. The NOL index was calculated from the extracted signals by the PMD-200 pain monitoring system. The NOL is based on a nonlinear combination of nociception-related physiologic parameters: HR, HRV (at the 0.15 to 0.4 Hz band power), amplitude of the photoplethysmography wave, skin conductance level, and their time derivatives15 obtained continuously using a non-invasive finger probe. The NOL is based on the advanced statistical and machine learning techniques to combine multiple signals into a single composite index. The NOL is a multiparameter nonlinear combination of HR, HRV, PPGA and SCL derived from random forest regression displayed on a scale from 0 to 100. Random forest is an algorithmic modeling approach that enables combining multiple parameters of different origin and discovering their complex nonlinear interactions16.
All study participants underwent the following protocol of measurements with the NOL index during their long COVID-19 follow-up consultation: step 1, five minutes lying down, step 2, five minutes standing, step 3, thirty seconds of flexion/extension and step 4, two minutes sitting down. This measure method shows many advantages as an easy and quick accessibility, a short recording time not disturbing the participant’s recovery and a lower sensitivity to breathing pattern than spectral variables17,18. Measures were performed each five seconds.
The study was approved by the Foch IRB: IRB00012437 (approval number: 20–12-02) on December 16, 2020. A non-opposed consent was obtained for all participants.
Parameters
The following clinical data were collected: age, gender, weight, height, body mass index (weight (kg) divided by height (m2)), heart rate, systolic, diastolic blood pressure, oxygen saturation, comorbidities (hypertension, diabetes and respiratory diseases), loss of taste and smell, previous oxygen therapy (administrated through low-flow nasal cannula), and duration from first symptoms of COVID-19 diagnosis.
Fatigue was defined by clinicians as at least two of the following criteria: loss of body mass exceeding 10%, NIJMEGEN superior or equal to 2319, PCL-5 test superior to 2020 and 30 s of up and down test inferior to 321.*
*I reviewed the footnotes in the above paragraph. It is not clear to me how the measures were used.
Results
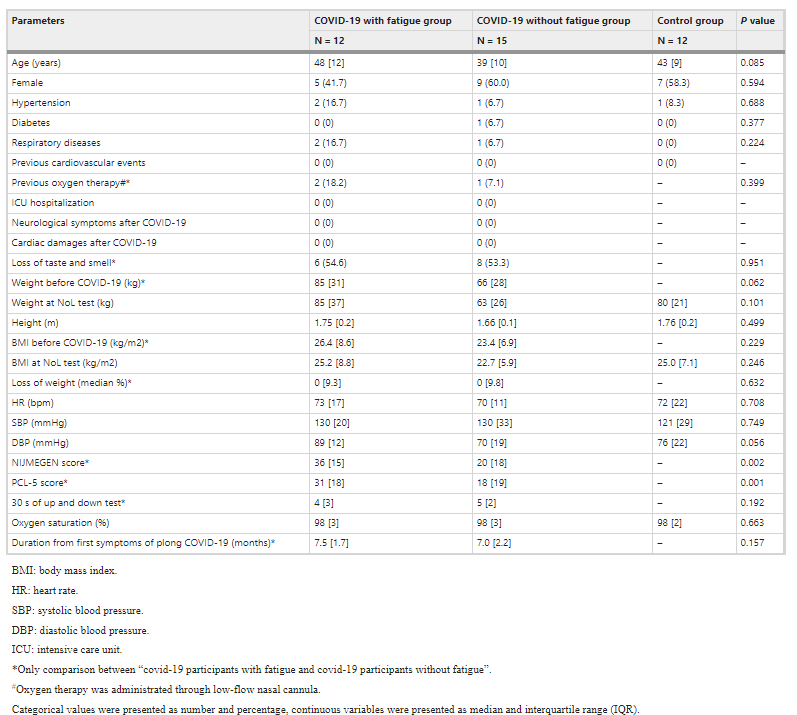
Characteristics of the participants were described in Table 1. Median average for age was 48 [12] years for patients with long COVID-19 with fatigue, 39 [10] years for patients with long COVID-19 without fatigue and 43 [9] years for the control group. Few patients of our study group presented comorbidities, only 3 patients with hypertension for long COVID-19 groups and one patient for control group, and only one patient with diabetes in long COVID-19 groups. No significant differences were observed for age (p = 0.085), gender (p = 0.594), comorbidities (hypertension (p = 0.688), diabetes (p = 0.377) and respiratory diseases (p = 0.224) between the three groups of the study population). 2 patients of the long COVID-19 group with fatigue and only one patient of the long COVID-19 group without fatigue were hospitalized and received oxygen therapy (p = 0.399). None of the participants of the study were hospitalized in ICU. 6 (54.6%) patients of long COVID-19 group with fatigue and 8 (53.3%) patients of the long COVID-19 group without fatigue presented loss of taste and smell (p = 0.951) (Table 1).
Results
Characteristics of the participants were described in Table 1. Median average for age was 48 [12] years for patients with long COVID-19 with fatigue, 39 [10] years for patients with long COVID-19 without fatigue and 43 [9] years for the control group. Few patients of our study group presented comorbidities, only 3 patients with hypertension for long COVID-19 groups and one patient for control group, and only one patient with diabetes in long COVID-19 groups. No significant differences were observed for age (p = 0.085), gender (p = 0.594), comorbidities (hypertension (p = 0.688), diabetes (p = 0.377) and respiratory diseases (p = 0.224) between the three groups of the study population). 2 patients of the long COVID-19 group with fatigue and only one patient of the long COVID-19 group without fatigue were hospitalized and received oxygen therapy (p = 0.399). None of the participants of the study were hospitalized in ICU. 6 (54.6%) patients of long COVID-19 group with fatigue and 8 (53.3%) patients of the long COVID-19 group without fatigue presented loss of taste and smell (p = 0.951) (Table 1).
Moreover, no difference was observed duration from first symptoms of long COVID-19 between the long COVID-19 participants with fatigue and thus without fatigue (respectively 7.5 [1.7] vs 7.0 [2.2], p = 0.157). Long COVID-19 participants with fatigue presented higher values of NIJMEGEN and PCL-5 scores (respectively, 36 [15] vs 20 [18] p = 0.002 and 31 [18] vs 18 [19], p = 0.001) but not for loss of body mass exceeding 10% (respectively 0 [9.3] vs 0 [9.8], p = 0.632) and the 30 s of up and down test (respectively, 4 [3] vs 5 [2], p = 0.192,) than long COVID-19 participants without fatigue. No neurological symptoms were reported during COVID-19 episode, except loss of taste and smell for 14 patients, but with no difference between the two groups (p = 0.951). No cardiac damage were reported by the patients (Table 1).
Discussion
As our data show, possible interesting clinical aspects arise when the population is stratified between fatigue and non-fatigue long COVID-19 patients. Our population presented no significant differences in comorbidities (i.e. hypertension and diabetes, previous oxygen therapy), hemodynamic parameters (i.e. blood pressure) and duration from first symptoms. We used NIJMEGEN score and PCL-5 score to discriminate patients according to fatigue status.
We observed that HRV, reflected by the NOL index, was significant different in long COVID-19 participants with fatigue compared to control participants. In our study, the NOL index*, a non-invasively measured multi-parameter index, was used to highlight the dysautonomia hypothesis in long COVID-19 participants. The variables that make up the NOL cover both sympathetic and parasympathetic activities of the ANS22. HRV is one of the main marker of dysautonomia12. HRV could be an important “window” for better understanding the inflammatory mechanism and neuroimmune system involved in long COVID-19 patients.
______________________________________________________________
*NOL (Nociception Level) is the technology and index developed by Medasense to objectively quantify a patient’s physiological pain response (nociception), enabling clinical teams to provide personalized pain treatment. NOL Technology. [This is a proprietary technology and the algorithm is unpublished.]
Recent but few experimental studies have shown the possible interest of HRV* as physiological measurement parameter for COVID-19 patients23,24. However, this non-invasive approach to evaluate the activity of the ANS remains too little understood and requires further investigations. Recognition of dysautonomia symptomatology in long COVID-19 patients could enhance the involvement of appropriate therapy.
________________________________________________________
Resuming Clinical characterization of dysautonomia in long COVID-19 patients
Recent but few experimental studies have shown the possible interest of HRV* as physiological measurement parameter for COVID-19 patients23,24. However, this non-invasive approach to evaluate the activity of the ANS remains too little understood and requires further investigations. Recognition of dysautonomia symptomatology in long COVID-19 patients could enhance the involvement of appropriate therapy.
____________________________________________________________
*Heart Rate Variability (HRV) from The Cleveland Clinic. Last reviewed by a Cleveland Clinic medical professional on 09/01/2021.
What is heart rate variability?
Heart rate variability is where the amount of time between your heartbeats fluctuates slightly. These variations are very small, adding or subtracting a fraction of a second between beats.
These fluctuations are undetectable except with specialized devices. While heart rate variability may be present in healthy individuals, it can still indicate the presence of health problems, including heart conditions and mental health issues like anxiety and depression.
References
- Buccelletti E, Gilardi E, Scaini E, et al. Heart rate variability and myocardial infarction: systematic literature review and metanalysis. (https://pubmed.ncbi.nlm.nih.gov/19694345/) Eur Rev Med Pharmacol Sci. 2009;13(4):299-307. Accessed 10/26/2021.
- Goessl VC, Curtiss JE, Hofmann SG. The effect of heart rate variability biofeedback training on stress and anxiety: a meta-analysis. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6466208/) Psychol Med. 2017;47(15):2578-2586. Accessed 10/26/2021.
- Lehrer PM, Gevirtz R. Heart rate variability biofeedback: how and why does it work? (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4104929/) Front Psychol. 2014;5:756. Published 2014 Jul 21. Accessed 10/26/2021.
- Shaffer F, Ginsberg JP. An overview of heart rate variability metrics and norms. (https://www.frontiersin.org/articles/10.3389/fpubh.2017.00258/full?fbclid=IwAR0OteHkGMXAo3uFNJwer9_of6ClJEIySmVjUz-cAJHAY8fNrGldhjhqUD0) Front Public Health. 2017 Sep 28;5:258. Accessed 10/26/2021.
- Shaffer F, McCraty R, Zerr CL. A healthy heart is not a metronome: an integrative review of the heart’s anatomy and heart rate variability. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4179748/) Front Psychol. 2014;5:1040. Published 2014 Sep 30. Accessed 10/26/2021.
- Soos MP, McComb D. Sinus Arrhythmia. (https://www.ncbi.nlm.nih.gov/books/NBK537011/) [Updated 2020 Nov 19]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Accessed 10/26/2021.
________________________________________________________
Resuming Clinical characterization of dysautonomia in long COVID-19 patients
Some etiologies may explain dysautonomia in long COVID-19 patients including neurotropism, hypoxia, and inflammation. However, it remains unclear whether dysautonomia associated with long COVID-19 results directly from autonomic-virus pathway or post-infectious immune-mediated processes.
COVID-19 infection could be responsible for invasion of the central nervous system (CNS) by a direct hematogenous and neural propagation25. COVID-19 virus in the airways could pass by the epithelial barrier invading the blood and lymph circulation and thus, propagate towards the CNS. The diameter of the COVID-19 virus is 60 to 140 nm, allowing it to pass through the blood–brain barrier (BBB) and gain entry into the CNS26. Other hypotheses highlighted a possible polarization of neurons leading to hyposmia due to conductive loss or neural loss27. Possible damages to the afferent hypoxia-sensing neuros could be due to the direct effect of COVID-19 by binding ACE2 expressed in capillary endothelium of BBB to gain access into the CNS28 or by indirect effect with cytokine storm on mitochondria or on nerve fibers29. Recent PET (positron emission tomography) scan findings have highlighted that COVID-19 neurotropism could occur in patients with impairment of olfactory bulb but also in other limbic structures, including thalamus/hypothalamus, cerebellum and the brainstem30,31. Moreover, the neuro-invasiveness of COVID-19 could have a direct role in hypoxia32. Excessive accumulations of acid metabolites in brain and anaerobic metabolites in mitochondria inducing edema and obstruction of the cerebral blood flow lead to hypoxia33.
The glossopharyngeal afferents, which innerve the carotid body and the vagal afferents enhancing the respiratory tract, present a key action in the monitoring organelle mechanism and modulating homeostasis by the stimulation of the ANS. Theses neurons are the primary sensory inputs of numerous reflex circuits modulating several major functions, such as HR, BP, and airway caliber34. Pulmonary receptors expressed on afferent vagal nerve terminals in the lung have mechanical or chemical stimuli, which translocate in the brainstem by small-diameter myelinated (Aδ) or unmyelinated (C)-fiber nerve axons. C-fiber afferents respond to inflammatory markers and could have a major role in prominent action in dyspnea and breath difficulty but also a major role in coughing34. Vagal C-fiber afferents innervate the larynx response to laryngeal discomfort while the afferent information arrives from the vagal and glossopharyngeal nerves to merge at the nucleus of the tractus solitarius (NTS), a key site of critical homeostasis pathway. Thalamus, somatosensory cortex, amygdala and insular cortex were implicated in breath perception. However, the biological phenomenon underlying the dissociation between hypoxemia and overt dyspnea remain unknown in COVID-19 patients. Nevertheless, the observed disassociation could be present in patients presenting lesions in the glossopharyngeal or vagus nerves due to cranial nerve damages4. Impairs of the HRV may be explained by the acute dysautonomia enhancing by afferent baroreflex failure. This mechanism leads to several damages at the afferent baroreceptor signaling, which starts from baroreceptors in carotid bodies to the vagal and glossopharyngeal nerve fibers, and then, to the NTS5.
One of the aspects of COVID-19 patients’ complications is the presentation of low blood oxygenation but no sensation of dyspnea29. This phenomenon has been called “happy”4,29 or “silent”35,36 hypoxemia. Nevertheless, this phenomenon is baffling to physicians and explanations remain unclear and hypothetic. This suggests that at least some sensory information could reach the brainstem to elicit a partial compensatory reflex respiratory response that is sufficient to lower the CO2 level, which diffuses more rapidly across the alveoli than oxygen. Respiratory pathology involves autonomic reflexes Projections from the brainstem to the cortex allow the brain to process homeostatic afferent signaling. A signal of internal hypoxia was received by the brain to ensure a rise of sensation of “air hunger” and needing to breathe, which is curiously absent in severe COVID-19 patients4.
Moreover, the ANS responds quickly to changes in physiological states, it may offer signals, in the form of HRV, that can warn of an impending cytokine storm sooner than other currently employed laboratory tests37. COVID-19 infection was associated with a cytokine storm characterized by the release of large amounts of pro-inflammatory cytokines and chemokines38,39. The relationship between HRV and inflammatory factors has been well extensively studied. Inflammatory factors might across the compromised BBB and cause brain damages. Thus, inflammation caused by viral infection could trigger and propagate chronic neuronal dysregulation40. A recent meta-analysis demonstrated an inverse relation between HRV and inflammation41. The measure of HRV was inversely correlated with CRP42. In the current COVID-19 infection, involvement of CRP became the vital monitoring patients’ inflammatory factor38,39. Nevertheless, the biological mechanism for the relationship between ANS and immune system interacted to impact the HRV has not been well understood37.
Conclusion
Long COVID-19 participants with fatigue may exhibit a dysautonomia characterized by dysregulation of the HRV, reflected by the NOL index, compared to control participants. Dysautonomia may explain the persistent symptoms observed in long COVID-19 participants, such as fatigue and hypoxia. Future clinical studies are needed to validate this hypothesis, with direct measurement of HRV and with specify focus on ICU or hospitalized patients, to allow better care of these participants during long COVID-19 rehabilitation.



