Note to myself: I made this post to remind myself to read that complete article on Imaging Protocols when I review this post. The article is outstanding.
In this post I link to and excerpt from the outstanding article Imaging protocols for CT chest: A recommendation [PubMed Abstract] [Full Text HTML] [Printable Full Text]. Indian J Radiol Imaging. Jul-Sep 2019;29(3):236-246.
Here are excerpts:
Abstract
Computed Tomography (CT) is the mainstay of diagnostic imaging evaluation of thoracic disorders. However, there are a number of CT protocols ranging from a simple non-contrast CT at one end of the spectrum, and CT perfusion as a complex protocol available only on high-end scanners. With the growing diversity, there is a pressing need for radiologists, and clinicians to have a basic understanding of the recommended CT examinations for individual indications. This brief review aims to summarise the currently prevalent CT examination protocols, including their recommended indications, as well as technical specifications for performing them.
Introduction
This review article aims to summarize the recommended thoracic CT protocols for various clinical/radiological indications including their technical parameters as well as applications of newer advancements in day-to-day clinical scenario based on current literature. The review does not address the status of ECG-gated cardiac/aortic CT. This manuscript was prepared as a part of initiative of Indian College of Radiology and Imaging (ICRI) to standardise imaging protocols in chest imaging.
The indication to perform a chest CT can be clinical, or based on an abnormality on prior imaging studies such as chest radiograph (CXR), fluoroscopy, MRI or abdomen CT. In almost all clinical scenarios, chest radiograph should be performed initially. Findings on CXR would help to tailor the appropriate CT examination. However, in several instances, CT will be performed even if the chest radiograph is normal e.g. Pyrexia of unknown origin (PUO). Hence, the use of the term clinico-radiographic indications is apt.
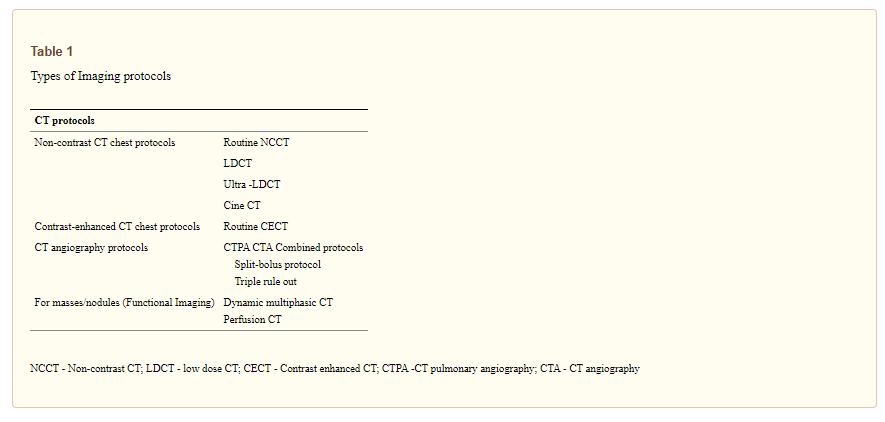
Broadly, the protocols may be divided into non-contrast CT (NCCT), contrast-enhanced CT (CECT) and then multiple modifications are available within this basic framework [Table 1]. Table 2 details the choice of CT protocol based on the clinico-radiographic indications. There are certain aspects of CT acquisition, though, which are common amongst all the protocols. Currently, all thoracic CT scans should be acquired in volumetric mode in full inspiration. Sequential mode may be used while acquiring limited expiratory scans. Certain clinical situations mandate the use of intravenous (IV) contrast such as evaluation of pyrexia of unknown origin (PUO) or acute infections. Omission of contrast in such scenarios can lead to inadequate evaluation of critical findings like mediastinal lymph nodes or complications.
t

Non-Contrast CT (NCCT) Chest Protocols
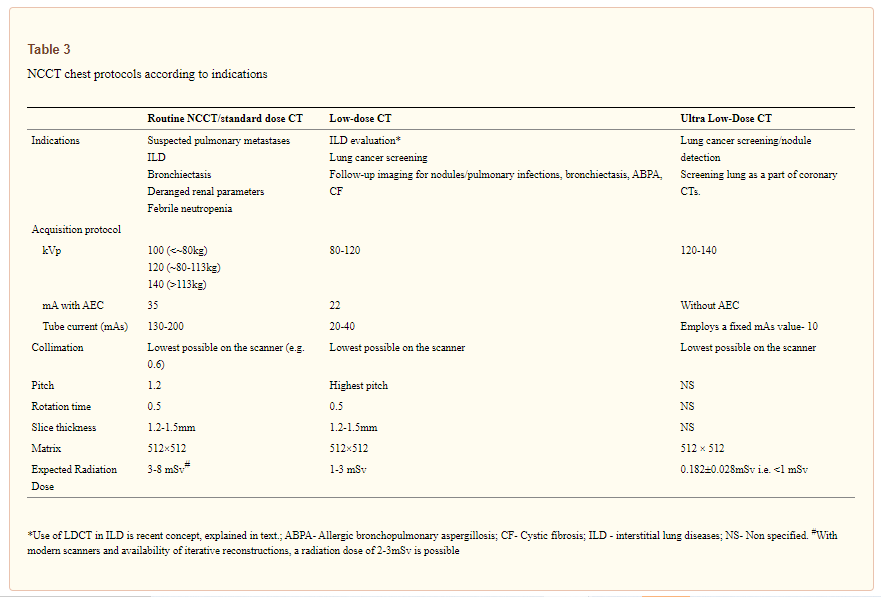
NCCT chest can be performed in various protocols such as routine NCCT in standard dose, low dose CT (LDCT) or Ultra-LDCT and their indications and technical parameters are summarized in Table 3.
Routine NCCT
Frequent indications of NCCT chest are suspected cases or follow up of metastasis, bronchiectasis, ILD and pulmonary infections.
Image acquisition
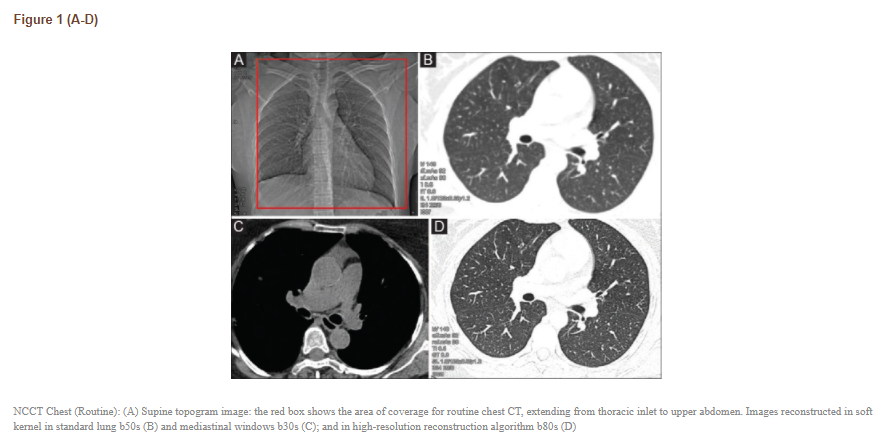
All non-contrast scans should be acquired in volumetric mode, scanning extending from thoracic inlet to caudally include upper abdomen [Figure 1]. Patients are imaged in supine position in suspended deep inspiration with arms extended overhead to reduce beam hardening artefact. Some modifications of the NCCT scans include expiratory and prone scans.