This post contains a link to and excerpts from CoreIM on 5 Pearls on Calcium Scores and Coronary CTAs [Links is to the podcast and complete show notes]. Posted: July 10, 2019
By: Dr. Evan Harmon, Dr. Pamela Douglas, Dr. Greg Katz, Dr. Martin Fried and Dr. Shreya P. Trivedi
Graphic: Dr. Caroline Srisarajivakul-Klein
Audio: Harit Shah
Peer Review: Dr. Aeshita Dwivedi, Dr. Matthew Vorsanger, Dr. Robert Doninno
Here are excerpts:
Time Stamps
- 3:10 What are the big picture differences of functional stress tests and anatomical cardiac tests?
- 7:48 What is coronary artery calcium scores’ role in managing coronary artery disease?
- 16:20 How do coronary CTAs compare to stress tests?
- 24:28 When should we avoid CTA?
- 29:33 How do we communicate coronary CTA results with patients?
- 36:02 Recap
Show Notes
Pearl 1
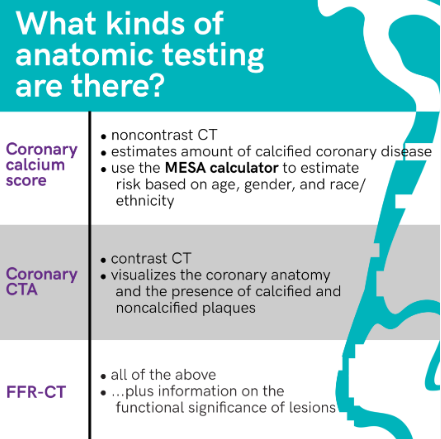
- Coronary CT is an evolving anatomical imaging modality that includes coronary calcium scoring and coronary computed tomography angiogram (CTA).
- In terms of information for risk stratification for coronary artery disease, anatomical tests provide information about plaque burden but does not reveal the physiological consequence of the atherosclerosis
Pearl 2
- Coronary calcium scoring should only be used to risk-stratify asymptomatic patients if the results may influence the initiation of primary prevention medications.
- Power of a calcium score of ZERO: statins are not associated with a reduction in major adverse events in this group and can consider discontinuing a statin.
Pearl 3
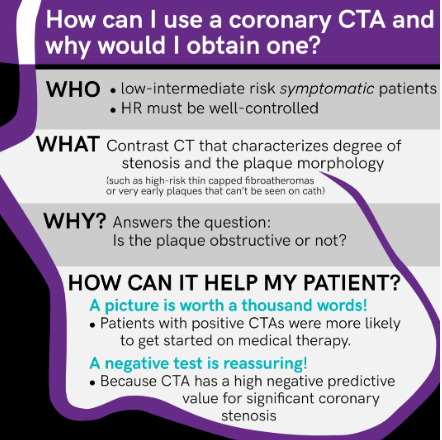
- Coronary CTA is simply a gated arterial phase contrast CT study that allows us to visualize the coronary arteries.
- We have randomized trial data that not only are these non-inferior to functional stress testing when it comes to death, myocardial infarction, hospitalization for unstable angina, or major procedural complication.
- There is the potential to reduce death and non-fatal MI using coronary CTAs over standard care.
- Patients undergoing coronary CTA as opposed to functional stress testing are more likely to be initiated on preventative, mortality-reducing therapies.
- Added benefits to coronary CT:
- Detect atherosclerotic disease that wouldn’t get picked up on with either stress test or even a coronary angiogram because it’s also not encroaching on the lumen
- Coronary CTA also picks up plaque morphology, such as with thin-cap fibroatheroma or “soft plaques”
- Coronary CTAs can also be used to identify congenital anomalies and are routinely done prior to afib ablations to evaluation pulmonary veins and sizing for aortic valves for TAVR.
Pearl 4
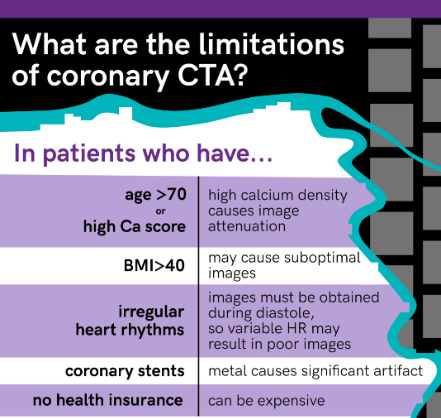
- Avoid coronary CTA in patients with elevated or irregular rates, frequent ectopy, or a history of prior stents. Also, it is generally a poor choice in the elderly or obese.
Pearl 5
- Coronary CTAs have a high negative predictive value and therefore, a CCTA without plaque burden can give reassurance that a patient’s symptoms are not from a cardiac source.
- Coronary CTAs with obstructive coronary lesions, the decision should be made on a case-by-case basis with the cardiologist regarding revascularization and/or optimizing medical therapy.