
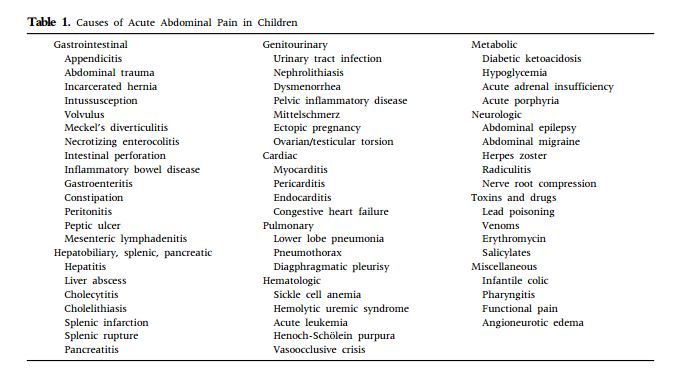
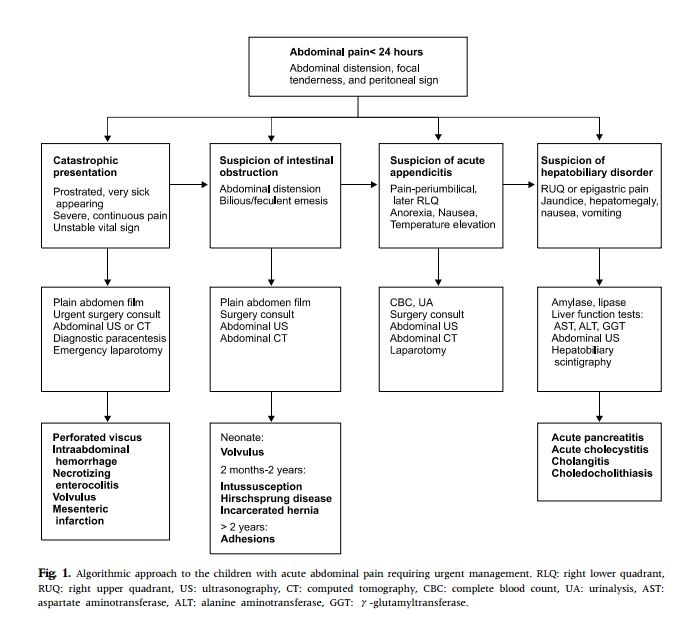
The following is from Reference (1):

The following is from Reference (2):
Most Common Diagnoses for Pediatric Abdominal Pain in the ED
In order of prevalence
1. Gastroenteritis
2. Respiratory Tract Infection (including Otitis Media, Pharyngitis and pneumonia)
3. UTI
4. Constipation
5. AppendicitisAside from gastroenteritis, upper respiratory tract infection is the most common diagnosis written at the bottom of the emergency chart for missed appendicitis in kids!
Pediatric Appendicitis Presentation
- The majority of cases of appendicitis in children <4y/o are perforated appendicitis, probably due to the atypical presentation and delay in diagnosis in this age group
- This delay in diagnosis is due to the absence of the classic history of anorexia and vague periumbilical pain followed by migration of pain to the right lower quadrant and onset of fever and vomiting in many children
- ‘Atypical is typical’ – diarrhea, constipation and dysuria are not uncommon and may lead the clinician astray; pain may localize to the back or psoas muscle as many children have a retrocecal appendix; vomiting may occur before abdominal pain (in contradistinction to the classic abdominal pain before vomiting in appendicitis) as younger children are unable to communicate their pain
- Clues to perforation: Diarrhea is more likely to occur after perforation and temp is often higher; no localization of pain with peritoneal signs; if there is abscess formation you may feel a mass in the RLQ
Physical Exam of the Abdomen Pearls in Pediatric Patients
- Children with appendicitis are usually lying still with the hips flexed as opposed to writhing in pain
- Examine the child in their caretaker’s lap, or lying on top of their caregiver, or with their legs wrapped around their caregiver’s trunk, first with their clothes still on
- Roll the patient’s hips and look for discomfort/pain with this maneuver Have the child palpate their own abdomen
Percuss before you palpate!
- Ask the child to ‘blow out the candles’ and look for respiratory splinting as the diaphragm lowers
- The equivalent of ‘jump tenderness’ in infants and toddlers is having the caregiver bounce the child on their knee and observing for irritability
- Examine the genitals of all boys with abdominal pain to look for testicular torsion!
Value of Lab Tests in Pediatric Patients with Abdominal Pain
- About 1/4 of children with gastro will have elevated WBC (because dehydration and acidosis elevate the WBC) and many children with appendicitis will have a normal WBC; however, if the appendix is perforated, the vast majority of children will have an elevated WBC count.
Clinical Pearl:
The earlier the presentation the less likely the WBC will be elevated.
The WBC is normal in first 24hrs in 80% of appendicitis cases.
- CRP may be more sensitive than WBC in identifying a perforated appendix but cannot rule out appendicitis
- Urinalysis (clean catch or catheter specimen): useful to rule out DKA, UTI, and pregnancy in teenagers as a cause for abdominal pain; sterile pyuria is consistent with appendicitis and gastro
- ‘Finger‐prick’ Glucose: hypoglycaemia in severe gastro, hyperglycemia in DKA
Clinical Pearl:
Pyuria and hematuria are findings that can be consistent with the diagnosis of appendicitis. Don’t let the findings of pyuria or hematuria dissuade you from diagnosing appendicitis in a child who you suspect has appendicitis clinically.
The following is from Reference (3):
Common causes of [Pediatric] Abdominal Pain
Notes:
- There is overlap between groups and classical symptoms may not be present; eg appendicitis in the preschool age group.
- Functional abdominal pain is very common but is a diagnosis of exclusion.
- Highlighted in red=time critical illness
Neonates Infants and Preschool School age child Adolescents Hirschprung’s enterocolitis
Incarcerated hernia
Intussuception
Irritable/unsettled infant
Meckel’s diverticulum
UTI
VolvulusAppendicitis
Gastroenteritis
Intussusception
Pneumonia
UTI
Volvulus
ConstipationAppendicitis
DKA
Gastroenteritis
Henoch Schonlein Purpura
Mesenteric adenitis
Migraine
Ovarian Pathology
Pneumonia
Constipation
Testicular torsion
UTI
Viral IllnessAppendicitis
DKA
Ectopic pregnancy
Cholecystitis/
Cholelithiasis
Gastroenteritis
Inflammatory Bowel disease
Ovarian cyst-torsion or rupture
Pancreatitis
Pelvic Inflammatory Disease
Renal calculi
Testicular torsion
UTI
Viral illness
Resources:
(1) Acute Abdominal Pain In Children [PubMed Abstract] [Full Text HTML] [Full Text PDF] 2013, Pediatric Gastroenterology and Nutrition.
(2) Episode 19 Part 1: Pediatric Abdominal Pain and Appendicitis from Emergency Medicine Cases.
(3) Guideline For Pediatric Abdominal Pain from The Royal Children’s Hospital of Melbourne
(4) Episode 19 Part 2: Pediatric Gastroenteritis, Constipation and Bowel Obstruction from Emergency Medicine Cases.
(5) Ultrasound First and the Pediatric Abdomen
(6) AIUM/SDMS Webinar: GI Sonography in the Pediatric Patient



